A Comprehensive Overview of Chronic Obstructive Pulmonary Disease (COPD)
By Dr Nabil Jarad PhD FRCP, Consultant Respiratory Physician
Posted 31 March 2026
11 Minute Read

Explore how smoking, occupational exposure, and comorbidities contribute to COPD and its role in respiratory disability claims.
Access our panel of 224 Respiratory Medicine Expert Witnesses >
An Introduction to COPD
COPD is a progressive disease characterised by airway obstruction. It is caused by exposure to noxious gas (mainly cigarette smokes). The disease is manifested with breathlessness and cough and have tendency to periods of exacerbations (flare ups).
Airflow obstruction is a fundamental part of the definition. It is defined as abnormalities seen on lung function tests mainly spirometry (figure 1).
Spirometry is a simple measurement of exhaled air volume measured in Litres against time measured in seconds. The two important components are Forced Expiratory Volume in the first second of exhalation (FEV1) and the Forced Vital Capacity (FVC) which the maximum exhaled volume.
Figure 1: Spirometer
A normal FEV1/FVC ratio is 70%-80%. COPD is regarded to be present when FEV1/FVC ratio is less than 70%. This pattern is called an obstructive defect, hence the obstruction termed into the COPD definition. Please see figures 2 and 3 for explanation.
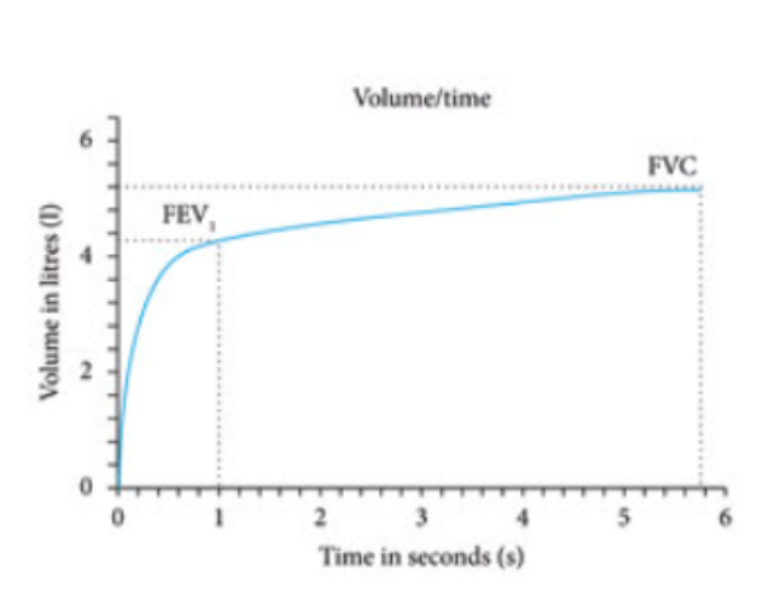
Figure 2: A normal spirometry. FEV1 is 4.1 litre and FVC 5.3 litre.
FEV1/FVC ratio is 77%
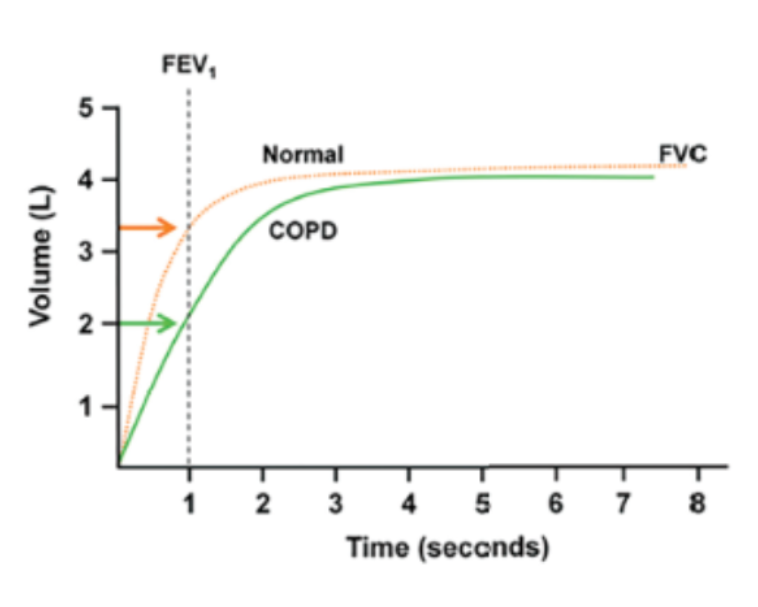
Figure 3: Normal Spirometry and COPD spirometry.
Orange line: A normal spirometry. FEV1 3.4 L, FVC 4.0 Litre. FEV1/FVC ratio is 85%.
Green line: COPD. FEV1 2.00, FVC: 3.9, FEV1/FVC ratio 51%.
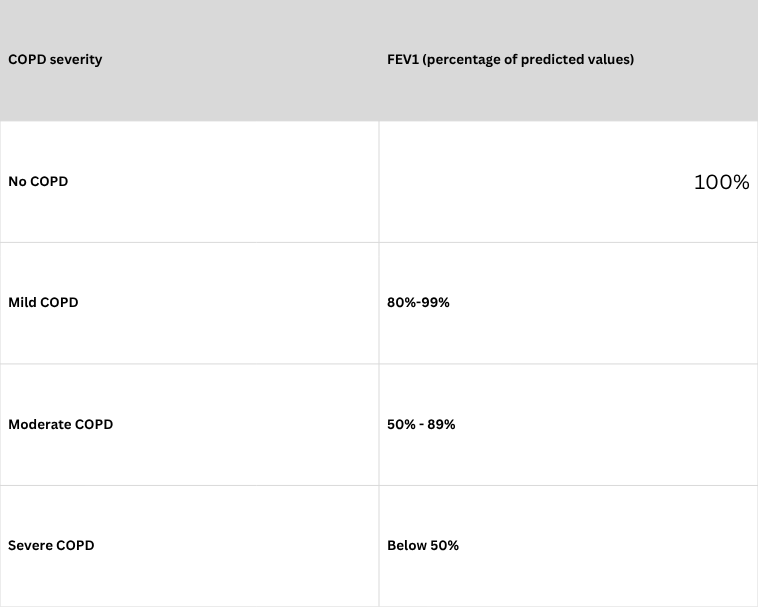
COPD severity:
Severity of COPD depends on the value of FEV1 estimated as a percentage of expected (predicted) value for the age, height and gender of the patients (please see below). Percentage predicted values are often calculated by the lung function machine. Please note that this is different from FEV1/FVC ratio.
Causes:
The commonest cause of COPD is cigarette smoking. A minimal degree of life-long smoking (the equivalent of 20 cigarettes a day for 10 years) is required for smoking to be associated with COPD.
COPD can also be occupational as a result of exposure to coal dust, silica dust and to cotton dust. Aging can also be associated with COPD.
Symptoms:
A combination of breathlessness, chest tightness, dry and productive cough, and increased tendency for chest infections are the three main symptoms of COPD.
In advanced disease, fatigue and ankle oedema ensued.
Types of COPD:
COPD could be mainly due to narrowing of the airway due to inflammation. This is associated with cough and sputum - this is called COPD with predominance of chronic bronchitis-type COPD.
It can also be due to lung tissue damage - this is called emphysema-type COPD.
Most patients would have a mixture of these two patterns, but with a predominance of either emphysema or chronic bronchitis.
Eosinophilic COPD has been recently recognised. This is a subtype of COPD in which blood eosinophiles increase. The importance of recognising this type is it can respond to oral and inhaled steroids. Newer biological agents are also effective in this sub-type of disease.

Figure 4: Emphysema-type COPD (left) and Chronic bronchitis type COPD (right).
The natural history of COPD:
This is illustrated in figure 4. Initial stages of COPD are seen around 40 years of age and manifest with cough and sputum (often called sputum cough).
As lung function declines, breathlessness ensues and increases with time. At a latter stages flare ups are encountered.
Restrictions of mobility due to breathlessness, low oxygen and no-pulmonary complications happen at the end stage of the disease
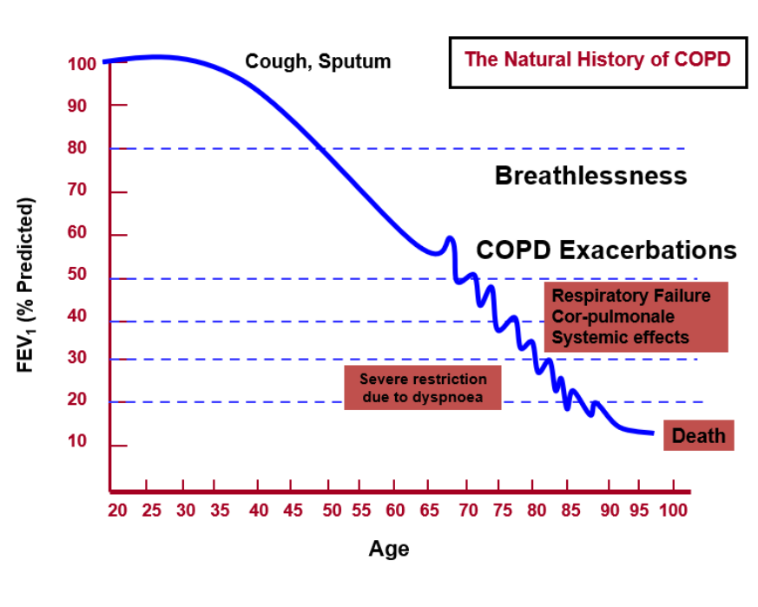
Figure 5: Lung function decline and clinical consequences in a typical COPD patient.
Systemic features of COPD:
Adding to cigarette smoking and age as risk factors, COPD patients are prone to impairment of functions of other organs.
The cardiovascular system is commonly affected. The incidence of heart attacks, angina and abnormal heart rhythm (atrial fibrillation) increases in COPD.
The rate of lung cancer, bladder cancer and oesophageal cancer increases with COPD.
Other diseases increase in COPD patients, including osteoporosis, type II diabetes and anxiety and depression (figure 6).
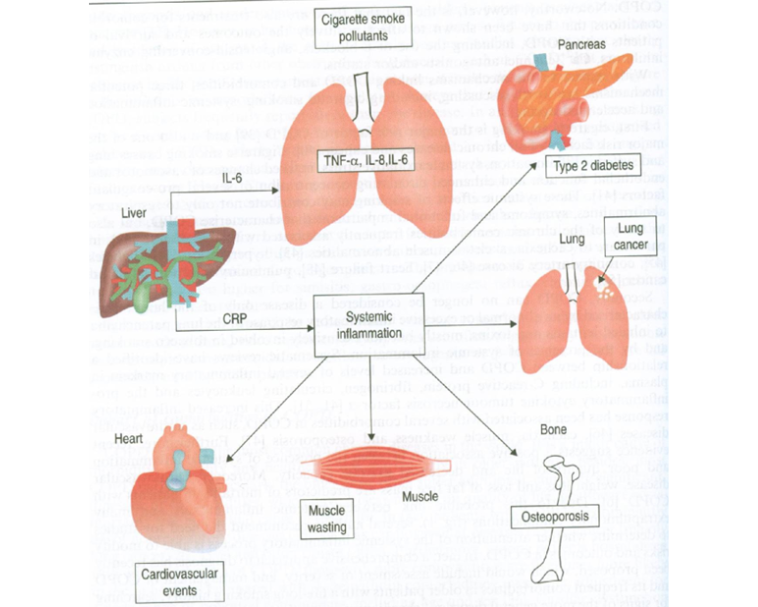
Figure 6: Systemic features of COPD
Exacerbation of COPD:
Exacerbation of COPD is an acute flare up of symptoms manifested by an acute increased symptom (cough and sputum). It is often induced by a viral or bacterial infection, and it requires antibiotics and oral steroids to treat.
The more frequent the exacerbation is the faster the decline in lung function tests and the shorter is life expectancy from the disease, [figure 7]. Therefore, strategies to reduce exacerbation is a common goal in the COPD community. These strategies include smoking cessation, steroid-containing inhalers, and winter vaccinations.
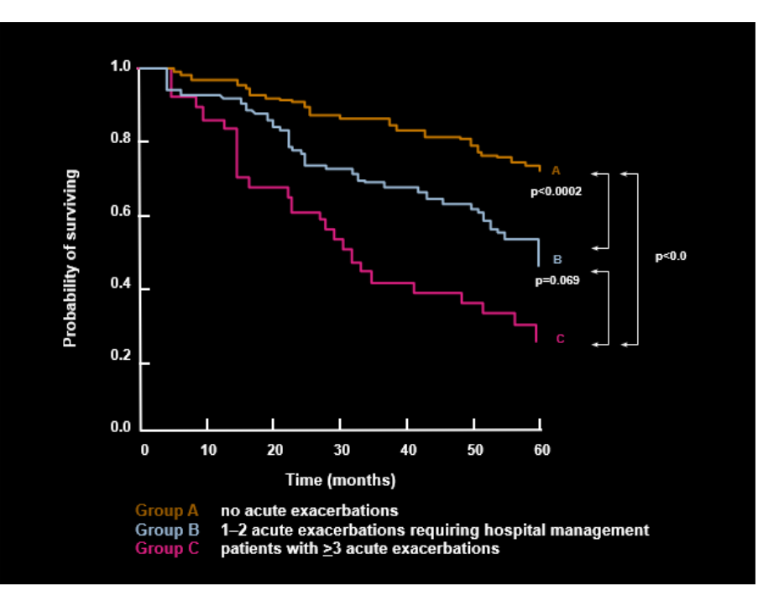
Figure 7: Probability of COPD survival is severely affected by increasing numbers of exacerbations.
Most Common Medical Legal Issues in COPD Patients:
Does the patient have COPD?
Answer: This would be easy if records of lung functions are available in the notes or if the patient attends a face-to-face consultation and undergone lung function during consultations with the expert.
If no lung function available, the diagnosis is made on balance of probability with symptoms, age and a history of cigarette smoking.
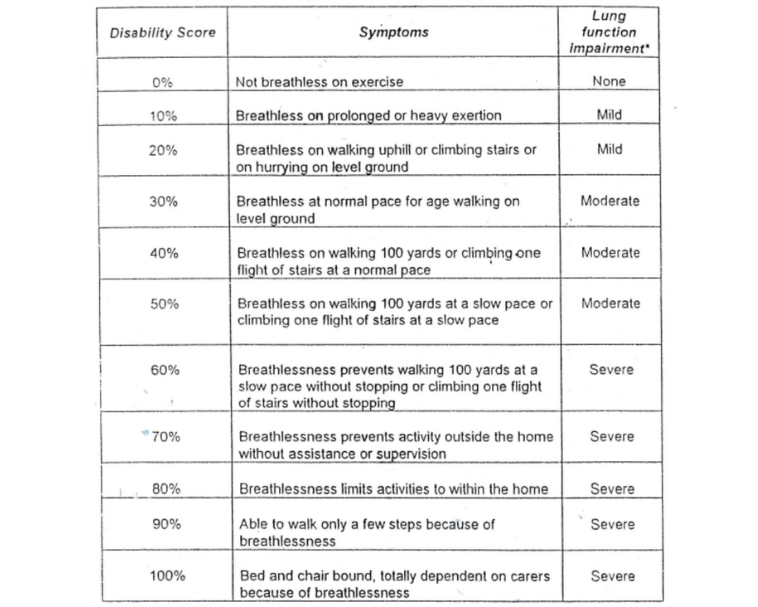
How is respiratory disability (severity) assessed in COPD?
Answer: The most used system of estimating respiratory disability is the one used during the coal miner’s compensation scheme 2000-2012. Disability depends on the degree of breathlessness as stated by the claimant and by their lung function impairment.
How can we apportion the respiratory disability if the claimant has conditions that cause respiratory disability such as COPD, cardiac disease and obesity?
Answer: This often needs information or is estimated. It depends on the severity of COPD, severity of heart failure normally on echocardiogram and on body mass index for obesity.
How would you estimate reduced life expectancy in COPD?
Answer: This depends on FEV1 and the age of patients. There are tables that give an excess mortality score in years. Generally speaking, the lower the FEV1 and the younger the age of the claimant the greater the excess mortality scores and the greater the reduction in life expectancy.
How would you apportion reduction in life expectancy in the presence of other life shortening conditions: heart failure and morbid obesity?
Answer: This estimate is similar to disability assessment, and it often follows the same pattern as disability assessment apportioning.
As Example:
A 60-year-old male patient who gets breathless upon walking 50 yards. His FEV1/FVC ratio is 65%. His FEV1 is 55% of his predicted values for his age and height.
He also has a heart failure diagnosed after a heart attack 10 years ago. His echo cardiogram shows a reduction of heart function by 50%.
He is obese, with body mass index of 38 (normal 20-25).
Answer:
Total respiratory disability is 60%.
His disability is apportioned as due to COPD 25% (looking at his FEV1), heart failure 25% (as per his echocardiogram results) and obesity 10% for his elevated body mass index.
But for his diseases, the life expectancy for a British Male is 80 years. This is expected to be shortened by approximately 10 years. The reduced survival rate is apportioned to be due to COPD 4 years, heart failure 4 years and obesity (and complication) by 2 years.
Management of COPD:
The aims of COPD treatment are to improve symptoms and quality of life, to decrease the number of exacerbations, to reduce the rete of decline in lung function and to improve survival.
The single most important factor that achieve all these aims is smoking cessation.
Inhaled bronchodilators improve symptoms and may be associated with reduced rate of exacerbations and improvement of survival.
Inhaled steroids are effective in reducing the rate of exacerbations and the rate of decline in lung function tests in patients with high eosinophil counts. Figure 8 shows some inhalers used in COPD.

Figure 8: Some inhalers used in COPD
In advanced stages when oxygen in the blood drops, oxygen therapy improves survival and may improve several aspects of impaired quality of life such as breathlessness and sleep impairment.
Pulmonary rehabilitation is a course of 6-8 weeks which requires attendance of around one hour twice a week. The course provides COPD education, management of symptoms including breathlessness and fatigue, encourages smoking cessation, and prescribes physical exercises.
The pulmonary rehabilitation courses improve quality of life, increase exercise tolerance and is associated with reduced number of exacerbations.
Winter vaccination is associated with reduced rates of chest infections.
Conclusions:
COPD is a progressive disease mainly induced by cigarette smoking. It manifests with breathlessness, cough and increased rate of chest infections.
Management is mainly in cigarette smoking. Inhalers and non-medicinal treatment such as smoking cessation, pulmonary rehabilitation improve symptoms, reduce exacerbations and improve survival.
COPD is associated with other diseases that increase symptoms such as cardiac disease and muscle and bone disease.
Oxygen therapy is provided in advanced stages in COPD, and it improve symptoms and increase survival.
The outlook of the disease has improved over the past 30 years with increase knowledge, increased rate of smoking cessation and with introduction of effective therapies.
About the Author:
Dr Nabil Jarad is a Consultant in General and Respiratory Medicine with over 20 years’ medico-legal experience, providing expert opinion in clinical negligence and personal injury claims involving respiratory disease.
He has prepared over 500 medico-legal reports and regularly advises on causation, condition progression, respiratory disability and life expectancy, particularly in cases involving COPD, occupational lung disease, asbestos-related conditions, tuberculosis and cystic fibrosis.
Dr Jarad has extensive experience in complex causation analysis, including apportionment between occupational and non-occupational factors, and has assessed thousands of cases through large-scale compensation schemes.
Alongside his medico-legal work, he is a Consultant Physician at Gloucestershire Hospitals NHS Foundation Trust and has previously held a Senior Lecturer post at the University of Bristol.
Tags:
- Causation
- Lung Cancer Delayed Diagnosis
- GP Negligence
- Cytology Screening
Expert Disciplines:
- Respiratory Medicine
About The Author

Dr Nabil Jarad PhD FRCP
Consultant Respiratory Physician
Dr Nabil Jarad is a Consultant Respiratory Physician with over 20 years’ medico-legal experience. He has produced 500+ expert reports and advises on causation, respiratory disability and life expectancy in clinical negligence and personal injury claims, particularly those involving occupational and chronic lung disease.
From the Blog
Related Articles
Essential reading for solicitors handling CHD claims - uncover key risks, missed follow-ups, and medico-legal pitfalls in adult congenital heart disease, with expert insight into real case examples.
Gain expert insight into the medical pitfalls behind delayed lung cancer diagnosis - vital for building stronger causation arguments and challenging standard-of-care in clinical negligence claims.

Identify missed opportunities in liver disease diagnosis with this expert guide - vital reading for clinical negligence solicitors handling delayed diagnosis, mismanagement, or failure to refer liver cases.
Find out why 70+ legal firms partner with INNEG.
Request a callback, or contact us.
INNEG respects your privacy. Any information you share with us will be used only to respond to your query.
Phone
+44 161 870 2461Thank you for your request!
We will get back to you as soon as possible.