Getting Epilepsy Right: Clinical Judgment and Medico-Legal Risk
By Dr Francesco Manfredonia, Consultant Neurologist & Clinical Neurophysiologist
Posted 09 April 2026
7 Minute Read
Avoid the common (and costly) pitfalls in epilepsy claims by understanding exactly where clinical judgment and documentation fail under legal scrutiny.
When epilepsy cases lead to complaints or claims, the same questions tend to recur: was the diagnosis correct; was treatment started appropriately (or not started when it should have been); were material risks explained adequately; and do the records show the clinician’s reasoning?
These issues matter to solicitors, treating clinicians and expert witnesses alike. Many epilepsy claims do not depend on complex technical disputes. More commonly, they stem from straightforward but significant failings: an incomplete history, undue confidence in the diagnosis, poor documentation, inadequate follow-up, or a failure to communicate and record risk clearly.
Seizure and Epilepsy are not the Same Thing
A seizure is a single event: a transient episode caused by abnormal electrical activity in the brain. Epilepsy is the underlying disorder: a predisposition to recurrent epileptic seizures.
The distinction is important. A person may experience a single seizure without having epilepsy. Conversely, epilepsy may be diagnosed after only one seizure if the predicted risk of recurrence is sufficiently high.
The ILAE practical definition of epilepsy includes:
- two unprovoked seizures more than 24 hours apart
- one unprovoked seizure where the risk of recurrence is estimated to be at least 60% over the next 10 years
- a recognised epilepsy syndrome. (ilae.org)
Accordingly, the diagnosis is not always a binary decision. It commonly involves clinical judgment informed by the history, examination and investigations.
Why the History Matters More than the Test Result
The diagnosis of epilepsy is primarily clinical. In practice, it depends chiefly on what occurred before, during and after the episode, and on any witness description.
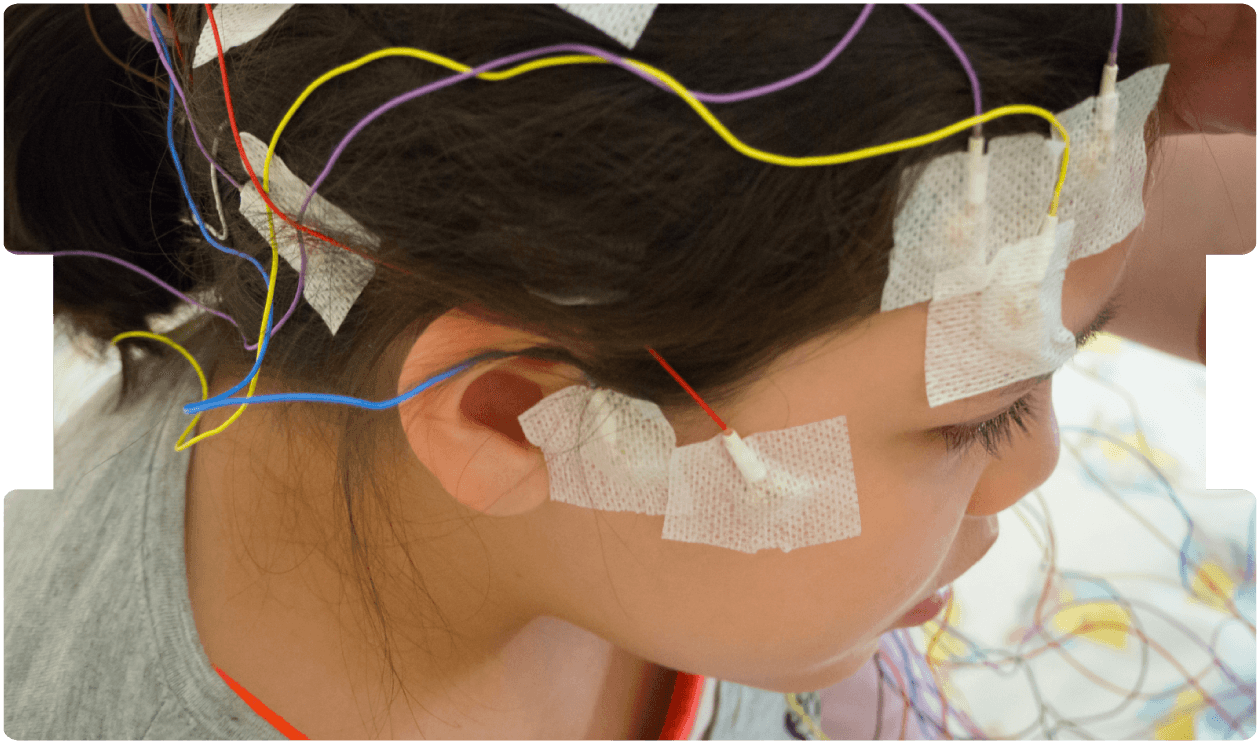
An EEG (electroencephalogram) records cerebral electrical activity using scalp electrodes. It can support the diagnosis by demonstrating abnormalities consistent with an increased propensity to epileptic seizures, but it does not diagnose epilepsy in isolation. EEG abnormalities can occur in people without epilepsy, and people with epilepsy may have a normal interictal EEG. An MRI scan may help by identifying structural pathology associated with increased seizure risk, such as gliosis/scarring, tumour, malformation or prior injury.
This is a common source of error. Where the history is limited but undue weight is placed on the EEG, a patient may be labelled as having epilepsy when the correct diagnosis is a mimic such as syncope, a sleep disorder, functional events, or migraine.
The First Seizure: When Should Treatment Start?
A first seizure does not, of itself, mean that anti-seizure medication should be started.
NICE advises that treatment after a first unprovoked seizure should not be offered routinely. It should be considered only in selected cases - for example, where features suggest a higher risk of recurrence (such as a focal neurological deficit, clear epileptiform abnormalities on EEG, or a structural abnormality on brain imaging), or where the overall risk is otherwise judged unacceptable. (nice.org.uk)
The evidence base is relevant. Early treatment can reduce the likelihood of further seizures in the short term (particularly over the next two years), but it does not appear to improve long-term remission. In practical terms, a neurologist may be justified either in starting treatment after a first seizure or in deferring it, provided the relevant factors are considered and the reasoning is clearly documented. (nice.org.uk)
From a medico-legal perspective, that is often the key point. The question is rarely simply “why did you treat?” or “why did you not treat?”. It is whether the clinician identified the relevant risk factors, discussed them with the patient, and recorded the decision-making process in a way that can be understood in retrospect.
Misdiagnosis Remains a Major Problem
Misdiagnosis remains a significant issue in epilepsy practice. The risk is greatest where the history is incomplete, no witness account is obtained, or alternative explanations are not properly explored.
The classic pitfalls are well recognised: events are labelled too quickly; EEG findings are treated as determinative when they are not; and the diagnosis is not revisited when subsequent events do not fit the original formulation.
A widely cited public example is the Leicester case involving Dr Andrew Holton. It concerned a large number of children who were incorrectly diagnosed with epilepsy, or treated for epilepsy when they did not in fact have it. In 2005, the High Court approved a settlement scheme for hundreds of affected children. The significance of the case lies not only in its scale, but in the pattern it illustrated: poor history-taking, excessive reliance on investigations, diagnostic overconfidence, and insufficient clinical challenge or oversight. (bmj.com; pmc.ncbi.nlm.nih.gov)
The Northern Ireland Independent Neurology Inquiry provides a related, broader lesson. It examined concerns arising from the practice of a neurologist whose patients later required large-scale recall and review. The final report, published in June 2022, made 76 recommendations. Its significance extends beyond any single diagnosis: it illustrates how clinical problems can persist for years when complaints, warning signs and patterns of substandard practice are not recognised or acted upon promptly within the wider system. (health-ni.gov.uk)
For expert witnesses, both examples are relevant because they illustrate two potential levels of causation: the individual consultation, and the governance and oversight framework around it.
SUDEP: What it is and Why it Matters
SUDEP stands for Sudden Unexpected Death in Epilepsy. It refers to the sudden and unexpected death of a person with epilepsy, where no other clear cause of death is identified after appropriate investigation. It is one of the most serious complications of epilepsy. (epilepsysociety.org.uk)
Not everyone with epilepsy carries the same level of risk. Risk is higher in certain groups, particularly people with ongoing generalised tonic-clonic seizures, especially where seizures are frequent, nocturnal, or overall control is poor. NICE notes that epilepsy is associated with an increased risk of premature death, including SUDEP, and recommends that this risk is discussed appropriately with people with epilepsy and, where relevant, their families and carers. (nice.org.uk)
From a clinical negligence perspective, SUDEP claims rarely depend on whether a clinician could have predicted an individual death. More commonly, they focus on whether risk was recognised, explained with appropriate sensitivity, modifiable factors were addressed, and the discussion was documented. This includes enquiry about seizure frequency, nocturnal seizures, adherence to medication, recent deterioration, and whether there were opportunities to improve seizure control. (nice.org.uk)
Where Negligence Claims Most Often Arise
In practice, the most common medico-legal problem areas in epilepsy include:
- misdiagnosis (particularly where syncope or other mimics were not properly considered);
- over-reliance on EEG;
- inadequate reasoning around treatment after a first seizure;
- failure to classify seizure type correctly;
- failure to advise and document driving restrictions;
- and failure to discuss, or act upon, SUDEP risk where clinically indicated.
These are rarely obscure mistakes; they are usually departures from basic clinical method.
Final Thought
The main lesson from epilepsy litigation is straightforward. Careful history-taking, proportionate use of EEG and MRI, clear reasoning about recurrence risk, and honest documentation of advice and uncertainty remain among the best safeguards for patients and clinicians.
That applies whether the issue is a first seizure, an incorrect diagnosis, a delayed review of deteriorating epilepsy, or a failure to address SUDEP risk appropriately.
Tags:
- Epilepsy Litigation
- Paediatric Epilepsy
- Seizure Mismanagement
- Seizure Risk
- Seizure Misdiagnosis
Expert Disciplines:
- Neurology
About The Author
Dr Francesco Manfredonia
Consultant Neurologist & Clinical Neurophysiologist
Dr Francesco Manfredonia is a Consultant Neurologist and Clinical Neurophysiologist with over 17 years’ experience and has been a medico-legal expert witness since 2022. He specialises in epilepsy and complex neurological conditions, and is Clinical Director at the Royal Wolverhampton NHS Trust. He combines clinical expertise with a strong focus on the psychological aspects of neurological care to support more holistic, patient-centred outcomes.
From the Blog
Related Articles

Gain expert insight into assessing post-traumatic seizure risk in head injury claims - vital for accurate prognosis, liability, and compensation in clinical negligence cases.

Neurology expert evidence is essential to clarify seizure types, genetic syndromes and treatment protocols, and to assess whether opportunities for earlier intervention were missed.

Misdiagnosed epilepsy can derail paediatric claims. In this expert webinar, Dr Mike Taylor shares how to spot red flags, prove breach, and strengthen causation in epilepsy-related clinical negligence cases.
Find out why 70+ legal firms partner with INNEG.
Request a callback, or contact us.
INNEG respects your privacy. Any information you share with us will be used only to respond to your query.
Phone
+44 161 870 2461Thank you for your request!
We will get back to you as soon as possible.