Medicolegal Dilemmas in Brain Cavernoma Diagnosis and Management
By Nitin Mukerji, Consultant Neurosurgeon
Posted 21 August 2024
6 Minute Read

Unclear on cavernoma cases? This blog breaks down the diagnostic pitfalls and treatment ambiguities that often lead to claims - vital reading for personal injury and clinical negligence solicitors.
By Mr. Nitin Mukerji, Consultant Neurosurgeon
This article delves into the medicolegal complexities of diagnosing and managing brain cavernomas.
These benign but diagnostically challenging lesions often lack specific guidelines, leading to potential medical legal claims.
The following will discuss the diagnostic difficulties, particularly in distinguishing cavernomas from other brain abnormalities, and the lack of consensus on treatment, emphasising the need for careful review and updated knowledge in legal evaluations.
Diagnostic Uncertainty
The uncertainty surrounding the diagnosis and management of cavernomas in the brain can result in a lot of medical legal claims.
These relatively benign lesions present a lot of diagnostic as well as management dilemmas, on which there is no specific guideline or consensus in the neurosurgery community.
A cavernoma is an abnormal cluster of blood vessels, primarily venous in nature which are found at different sites in the brain and typically has a raspberry like appearance.
Cavernomas are also called cavernous angiomas and cerebral cavernous malformations. They may or may not be associated with adjacent developmental venous anomalies.
Incidental Findings
A significant number of the cavernomas are incidentally discovered on scans for different reasons. Symptomatic cavernomas could present with small bleeds, seizures or chronic headaches.
Other specific symptoms could very well be related to the location of the cavernoma. In general, the bleeding associated with cavernomas is low pressure and most often non-life-threatening.
Multiple cavernomas can occasionally be associated with the CCM genes.
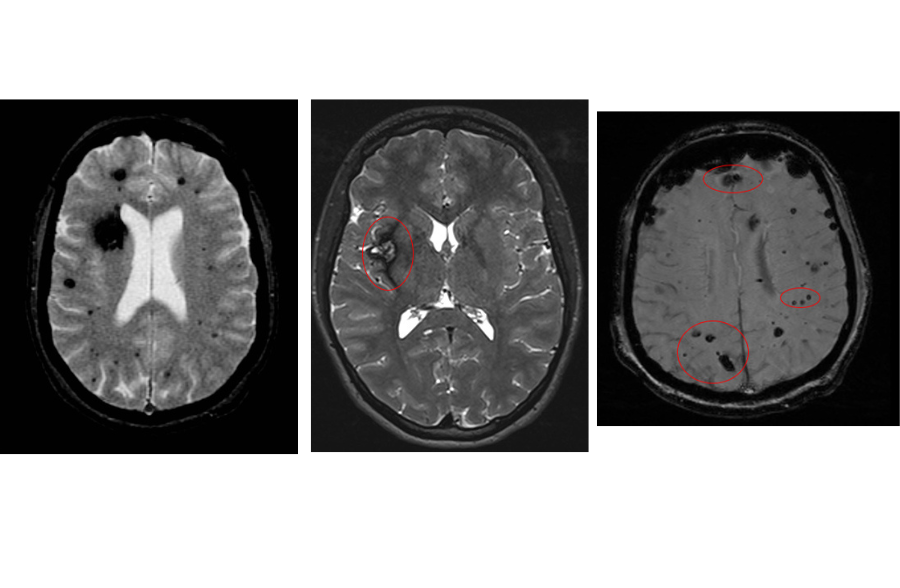
Cavernomas are difficult to diagnose on a CT scan but can be diagnosed on an MR scan.
On an MR scan, cavernomas can mimic meningiomas and even gliomas with small amount of haemorrhage around them.
When the diagnosis is not clear due to the presence haematoma, repeat scanning when the blood load has resolved or reduced is recommended.
It is also not uncommon to find a different histological lesion when operating with the expectation of finding a cavernoma.
Management
Purely incidental cavernomas generally are managed conservatively as the risk of haemorrhage is quite low and most neurosurgeons would agree that the literature overestimates the risk of primary haemorrhage.
Once the cavernoma presents with a bleed, the risk of repeat haemorrhage is higher and therefore a discussion needs to be had with the patient with regards to further treatment and this could be either surgical or with stereotactic radiosurgery.
Surgery is generally reserved for lesions that are superficial, non-eloquent and surgically accessible.
Deeper cavernomas generally tend to be managed either conservatively or with stereotactic radiosurgery.
Notably the efficacy of stereotactic radiosurgery for cavernomas is lower than that for an arteriovenous malformation.
To understand how surgical decision-making and MDT discussions intersect with legal scrutiny, read our insights on brain surgery and the Montgomery Dilemma.
Diagnostic Challenges
The medical legal dilemmas in cavernomas arise primarily from fact that the diagnosis at times from imaging is not apparent and meningiomas or gliomas can be mistaken for cavernomas.
For further exploration of diagnostic ambiguity in neuro-oncology claims, see our blog on the complex and uncertain landscape of brain tumours in medicolegal practice.
Follow-up and serial imaging generally is not of great value unless it is for multiple cavernomas associated with the CCM gene but there is no specific agreement on this either.
In such scenarios management generally is dictated by repeated haemorrhage, progressively worsening neurology or uncontrolled seizures rather than true change in imaging features which therefore makes serial follow-up scans redundant.
Treatment Options Evaluated
It is also worth noting that there is no specific treatment which is universal and better and there are currently ongoing randomised trials to see if any of these treatment options performed better than conservative management alone.
Microsurgical removal is supposed to be the most effective as it has the greatest chance of complete excision.
Surgery for cavernomas can be quite tricky as the lesions are small and be difficult to localise even with careful neuro navigation and use of intraoperative ultrasound.
In these circumstances, if due diligence and careful consideration has been applied at all stages, missing a cavernoma intraoperatively despite all measures is something that has been reported frequently.
Even after a satisfactory complete resection, postoperative scans are often reported as showing residual cavernoma, but this is more often due to haemosiderin staining of the cavernoma cavity rather than true residual cavernous malformation.
Review
All these aspects and the lack of clear guidance on the management makes it very important for medical legal experts to carefully review the notes and imaging in great detail and keep up to date with the current literature before any specific opinion is expressed.
Fundamental and basic sciences research into the pathogenesis of cavernomas also continues at great pace and it is vital for experts to keep abreast of these developments so that the most current knowledge is used to formulate the opinions.
About the Author
Mr. Mukerji is a consultant neurosurgeon specialising in cerebrovascular and skull-base surgery at The James Cook University Hospital, Middlesbrough.
He also acts as a clinical information officer for the trust and serves as editor-in-chief of the British Journal of Neurosurgery.
Additionally, he holds honorary consultant roles at; County Durham and Darlington NHS Trust, Imperial College London NHS Trust, Newcastle upon Tyne NHS Trust, and is an honorary fellow at the Wolfson Research Institute, Durham University.
To request his CV or for any medico-legal matters she can be reached at nitinmukerji@inneg.co.uk
Tags:
- Cavernoma Negligence
- Brain Cavernomas
- Diagnostic Uncertainty
- Cerebral Cavernous Malformation
- Neurosurgeon Expert Witness
Expert Disciplines:
- Neurosurgery
About The Author

Nitin Mukerji
Consultant Neurosurgeon
Mr. Nitin Mukerji is a Consultant Neurosurgeon at The James Cook University Hospital, specialising in cerebrovascular and skull-base surgery. He also serves as Clinical Information Officer for the trust and is Editor-in-Chief of the British Journal of Neurosurgery. Mr. Mukerji holds honorary consultant roles across multiple NHS trusts and is an honorary fellow at Durham University’s Wolfson Research Institute. He provides expert witness services in neurosurgery.
From the Blog
Related Articles

Gain expert insight into cerebral visual impairment (CVI) to better assess causation, prognosis, and lifelong impact in paediatric brain injury claims.

Sharpen your approach to complex claims involving functional symptoms. This expert-led guide helps distinguish genuine neurological disorder from malingering - crucial in high-stakes cases.
For clinical negligence solicitors, this expert insight on atrial fibrillation clarifies diagnosis, risk factors, treatment, and medico-legal nuances-helping build stronger, evidence-based claims and defenses.
Find out why 70+ legal firms partner with INNEG.
Request a callback, or contact us.
INNEG respects your privacy. Any information you share with us will be used only to respond to your query.
Phone
+44 161 870 2461Thank you for your request!
We will get back to you as soon as possible.