Missed Periodontal Disease: Clinical Oversights and Medico-Legal Consequences
By Dr Ravinder Varaich, Principal Dentist & Expert Witness
Posted 17 February 2025
9 Minute Read

Failing to diagnose periodontal disease can be a costly oversight. This blog offers solicitors clear guidance on identifying breaches, assessing causation, and strengthening dental negligence claims.
By Dr. Ravinder Varaich, Principal Dentist
This article examines key aspects of periodontal disease claims, emphasising the importance of accurate diagnosis, thorough record-keeping, and adherence to treatment guidelines.
If you're new to handling dental claims, our beginner’s guide to navigating dental personal injury claims offers a practical starting point for understanding the fundamentals.
Dr Varaich addresses the role of patient lifestyle factors and common breaches in dental duty, focusing on how both practitioner actions and patient habits contribute to the progression and management of periodontal disease.
Aetiology of Periodontal Disease
Periodontitis is a chronic inflammatory disease of bacterial origin that affects the supporting tissues around the teeth.
The disease is initiated by the accumulation of plaque, which is a biofilm composed of bacteria and their products on the tooth surface.
A host’s immune response to the bacterial challenge is responsible for the destruction of the periodontal tissues.
Severity of the disease is influenced by various factors, such as smoking diabetes, and genetic predisposition.
The risk to the disease can be reduced by maintaining good oral hygiene, and regular dental examinations.
According to the 2009 UK Adult Dental Health Survey indicates 37% of the adult population suffers from moderate levels of chronic periodontal disease (with 4-6mm pocketing), while 8% of the population suffers from severe periodontitis (pocketing exceeding 6mm).
Periodontal disease is a slowly progressing disease, and bone loss occurs over a period of years.
Therefore, a case of periodontal disease should include records as far back as possible in order to establish when the disease is likely to have begun, and the pattern of progression.
Periodontal cases are usually multifactorial, and involve numerous dentists over a period of years, and causation is usually split between numerous defendants.
Breaches Of Duty
As healthcare providers, dentists are expected to screen, diagnose and manage periodontal disease.
Failure to do so is a breach of duty.
Any negligence case is generally split into pre treatment assessment and consent, treatment and aftercare.
The minimum standard of care is a periodontal screening tool, the BPE score (basic periodontal examination).
Screening involves probing of the gums and scoring according to the presence of bleeding on probing, presence of plaque and calculus deposits, and the depth of pockets present.
Failing to perform basic periodontal screening is a breach of duty.
The 2009 UK Adult Dental Health Survey indicates 37% of the adult population suffers from moderate levels of chronic periodontal disease (with 4-6mm pocketing), while 8% of the population suffers from severe periodontitis (pocketing exceeding 6mm).
The below table taken from the British Society of Periodontology shows the codes and what they represent.
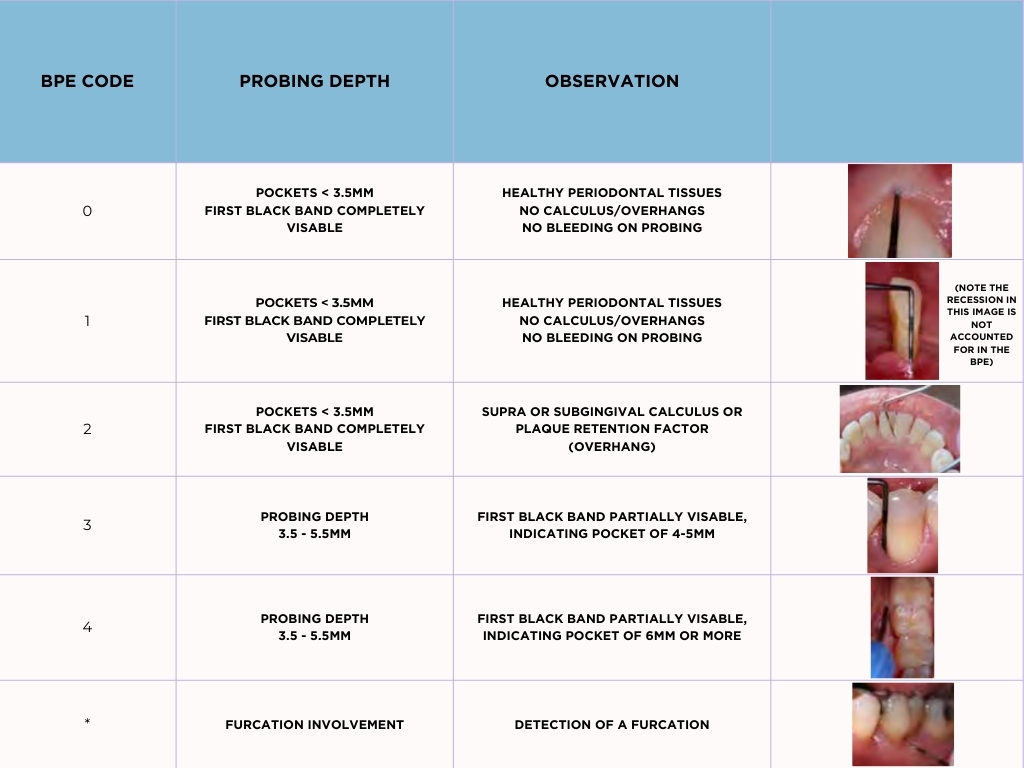
British Society of Periodontology guidelines state a BPE examination should be performed at every examination appointment.
Patients scoring codes of 3 or 4 require a more detailed periodontal pocket charting, as well as radiographs showing bone levels around the affected teeth.
British Society of Periodontology Guidelines
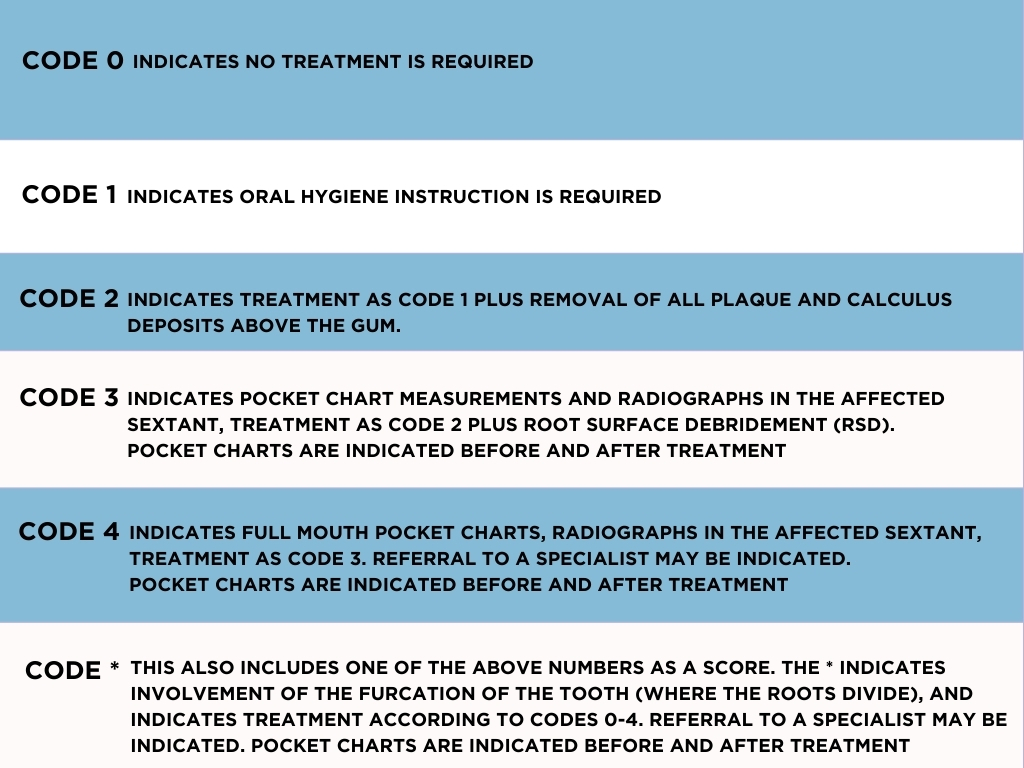
The BPE code indicates the treatment required as noted in the table above.
Failures to perform the treatment indicated for each score is a breach of duty.
It is the dentist’s responsibility to establish a diagnosis in accordance with the 2017 classification.
The above BPE scores and where relevant pocket measurements, bleeding on probing and radiographs are required to establish this diagnosis.
Failure to do appropriately diagnose the patient is a breach of duty.
Patient Factors
The patient also has a responsibility to ensure they follow advice given, such as recall intervals of attendance, following oral hygiene advice, smoking cessation, and management of their general health.
Sample Periodontal Disease Case
The Claimant's Summary:
42 year old Mrs. A has attended the same practice for 20 years.
More recently, she complained of bad breath, bleeding gums and was starting to note her teeth were drifting.
She was a smoker, smoking 20 a day since the age of 15, had poorly controlled diabetes, and reports she was told by her dentist that she had gingivitis and she was told she should brush better and floss, but was shocked when she attended a new dentist that she had severe bone loss and would likely lose her teeth within the next 5 years which upsets her greatly as she saw her mother lose her teeth at a young age and struggle all her life with dentures.
She enjoys singing in her local choir and plays the saxophone, and does not want to wear dentures as she feels it will affect her ability to sing and use the saxophone.
Upon the advice of her dentist, she has stopped smoking, improved her oral hygiene, and now flosses and uses inter-dental brushes 2 x daily.
Her pocket measurements have reduced significantly, and she now attends every 3 months to see the hygienist.
However, it is too late for a number of her teeth, and she wants to know whether she has a case for negligence.
The Dental Records
The records of the practice are very brief with historical records being typical of the below note:
Exam, c/o bleeding gums
Poor OH, OHI given
BPE
121
222
Bitewings: NAD
Diagnosis: Gingivitis
Risks, benefits discussed consent given.
S/P done
TCA 6 months
Radiographs over the years show a progression of bone loss.
Pre treatment assessment and Consent
There was a failure to appropriate screen for periodontal disease in accordance with BSP (British Society of Periodontology) guidelines. The records show scores of 1s and 2s throughout the period of care, and considering the bone loss noted, there is clear inaccuracy in the BPE scores.
Considering the assertion of inaccurate BPE scores, there are failures to perform pocket measurements, and appropriate radiographs were not taken as not all bone levels are visible on the radiographs taken.
There was a failure to record bleeding on probing after 2018 in accordance with BSP guidelines.
There was a failure to note bone loss on the radiographs in line with record keeping guidelines (General Dental Council and FGDP guidelines). There was also a failure to discuss the radiographic findings with the patient.
Considering the bone loss, the diagnosis of gingivitis was noted to be inappropriate as this does not consider the bone loss, and therefore presence of periodontal disease. There was therefore a failure to diagnose periodontal disease.
From 2018 onwards there was a failure to diagnose the periodontal disease in accordance with the 2017 BSP guidelines.
There was a failure to consider and manage the patient’s risk factors to periodontal disease, namely, there was a failure to provide appropriate oral hygiene advice and discuss the role of plaque in the aetiology of periodontal disease. Though it is noted in the records OHI given, there is no evidence specific and tailored advice was provided to the patient, such as frequency and technique of toothbrushing, frequency and technique of flossing and use of inter-dental brushes. There were failures to determine genetic factors (the patient’s mother lost her teeth at an early age) meaning the patient was at a higher risk of developing the disease, failure to discuss smoking cessation, and the role of smoking in the aetiology of periodontal disease, failed to discuss the role of diabetes and consider referral to the GP.
Considering the progression of bone loss, and patient age at the time of bone loss, there was a failure to consider referral to a specialist.
Though the records state “risks, benefits discussed, consent given”, there is no evidence of what risks, and what benefits were discussed, and considering the records are the same for each examination entry, it is inferred a template was used, and these discussions are not likely to have taken place. Considering the above failures, and as the patient was not appropriately screened and diagnosed, the consent is not valid.
Treatment
Considering the breaches of duty in the accuracy of the BPE scores, the treatment of scale and polishing is not in line with the BSP guidelines.
Namely, there was a failure to record periodontal pocket measurements and failures to perform root surface debridement.
After Care
Considering the bone loss, risk factors and presence of periodontal disease, the recall interval of 6 months is not appropriate.
There was a failure to perform post treatment pocket measurements.
Knowing how to select the right expert is crucial - our guide to finding and instructing a dental expert can help ensure you have the strongest foundation for your claim.
About the Author
Dr. Ravinder Varaich is a Principal Dentist and Expert Witness with over 20 years of experience in general and cosmetic dentistry. Originally qualifying in 2002, she has provided expert witness services since 2006.
Dr. Varaich has undergone specialist expert witness training with Bond Solon, completing the University of Cardiff qualification in expert report writing.
Her areas of expertise include general dentistry, periodontics, root canal treatments, crowns, bridges, veneers, extractions, implants, and orthodontics.
For medico-legal enquiries or to request her CV, Dr. Varaich can be reached at ravindervaraich@inneg.co.uk.
Tags:
- Periodontal Disease
- BPE Scoring
- Dental Negligence
- Periodontist Expert Witness
- Oral Hygiene
- Bone Loss
- Inaccurate Diagnosis
- Dental Litigation
Expert Disciplines:
- Dentistry
About The Author

Dr Ravinder Varaich
Principal Dentist & Expert Witness
Dr. Ravinder Varaich is a Principal Dentist and Expert Witness with 20+ years’ experience in general and cosmetic dentistry. Since 2006, she’s provided expert reports, trained in expert witness skills at Cardiff University and Bond Solon. Her expertise covers periodontics, root canals, crowns, implants, orthodontics, and more.
From the Blog
Related Articles

Unlock expert insights to strengthen your clinical negligence dental claims. Dr. Varaich’s guide offers practical tips to secure detailed, accurate dental reports - helping you build stronger cases and achieve better outcomes.
Gain expert insights on hip replacement positioning to strengthen clinical negligence cases. Mr. Shaw’s guide helps you assess implant claims with confidence and improve case outcomes.

Unlock expert insights for dental clinical negligence claims with this practical guide. Learn how to choose, instruct, and collaborate with dental experts to strengthen your cases and save time.
Find out why 70+ legal firms partner with INNEG.
Request a callback, or contact us.
INNEG respects your privacy. Any information you share with us will be used only to respond to your query.
Phone
+44 161 870 2461Thank you for your request!
We will get back to you as soon as possible.