Implant Misplacement: Legal Considerations for Solicitors
By Mr. David L Shaw, Consultant Orthopaedic Surgeon
Posted 16 January 2024
10 Minute Read

Gain expert insight into how implant positioning, leg length, and imaging affect hip replacement outcomes - and the clinical negligence claims that can follow.
By Mr. David Shaw, Consultant in Orthopaedics & Trauma
The aim of hip replacement surgery is to give the patient a pain free hip joint which restores or maintains leg length and is not vulnerable to dislocation. In this article I will discuss how orthopaedic surgeons judge whether a replacement hip joint has been inserted correctly.
Acetabulum - Hip Socket
When a new hip socket is fitted inside the natural socket, the ball part of the joint is smaller than the native hip, which increases the risk of dislocation. Correct positioning of the socket can help reduce this risk. Think of the socket as an umbrella, where the handle of the opened umbrella represents the axis of the socket.
Orthopaedic surgeons use two terms to describe the orientation of the socket or its "handle":
Version
Inclination
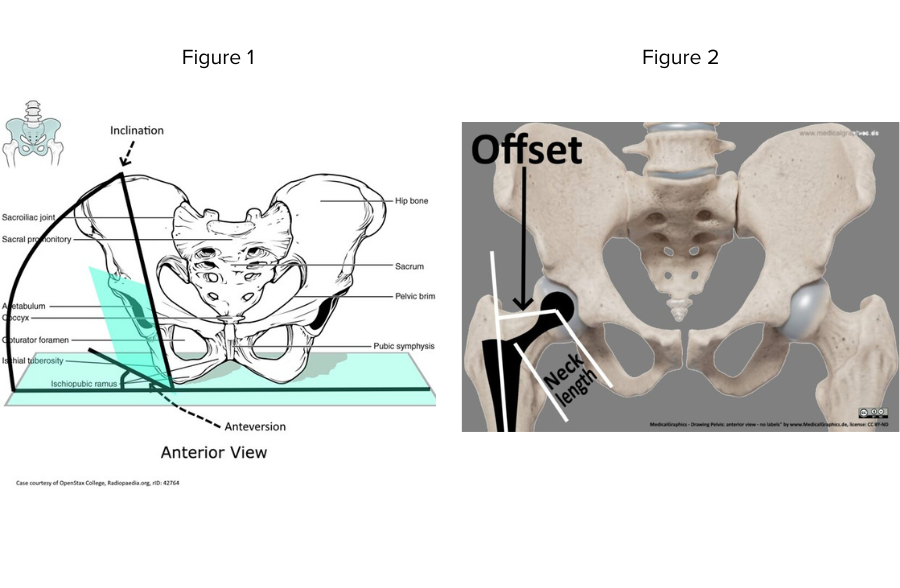
In Figure 1, it can be observed that the natural hip socket faces forward (anteversion), and the artificial replacement can be placed in normal or neutral anteversion, excessive anteversion, or retroversion/retroverted. A retroverted socket increases the risk of posterior dislocation when the leg is turned inwards, while excessive anteversion increases the risk of dislocation when the leg is turned outwards. The inclination of the socket refers to the degree to which the axis points downwards. The terms "open" and "closed" are often used, with an open socket being more vertically placed than its closed counterpart. An overly vertical socket increases the risk of dislocation as the knee is brought towards the midline (adduction).
The acceptable range of these two measures are often referred to as the "safe zone," which suggests that the risk of dislocation is reduced when the socket is placed within this zone. However, it is important to note that in clinical practice and clinical negligence, this concept is a simplification. Many hip replacements with seemingly poor socket positioning function normally, while some patients with apparently well-positioned components experience instability and dislocation. Hip joint stability is influenced by other factors, including the competence of the supporting soft tissues and the size and positioning of the femoral (thigh bone) component.
Femoral Component:
Similarly to the socket, the thigh bone component, which provides the ball of the artificial joint, is slightly pointed forwards (antervertion). Excessive anteversion increases the risk of dislocation when the leg is turned outwards, while retroversion increases the risk of dislocation during internal rotation. An anteverted femoral component may compensate for a retroverted acetabulum, and vice versa.
Leg Length / Neck Length & Offset:
Lengthening the leg at the hip joint generally tightens the soft tissues and reduces the risk of dislocation. Restoring leg length is a necessary part of the surgery, especially since arthritis itself shortens the leg at the hip joint and restoring length aids long-term stability. However, excessive lengthening can result in noticeable limb length discrepancy after surgery, which is one of the common causes of clinical negligence claims. Shorter female patients are more sensitive to limb length discrepancy compared to taller male patients. The length of the implant's neck (neck length) and the distance between the ball centre and the thigh bone (offset) independently contribute to joint stability and also affect leg length (figure 2).
Surgeons strive to balance the risk of overlengthening to avoid dislocation with the risk of limb length discrepancy. This requires skill and experience, and intraoperative measurement of leg length is just one factor in achieving this balance. Assessing the tightness or looseness of the hip joint in an anaesthetized patient and predicting how the patient will feel when awake requires considerable skill and judgment. While limb length discrepancy is often assumed to be the cause of postoperative dissatisfaction, increased offset (which is invisible by external examination) can also be a significant factor contributing to the subjective feeling that the hip is "not right."
A Word About Imaging:
Assessing implant positioning requires radiographic image analysis, which may include the following:
Scaled pre and postoperative pelvic radiographs
Lateral hip radiographs
Leg alignment (limb length) radiographs
CT scan of the pelvis
CT scan for rotational lower limb profile measurement (including both hips, knees, and ankles)
Detailed radiographic analysis using dedicated image viewing software and hardware in a diagnostic environment is necessary to determine breach of duty of care and causation in assessing implant positioning. It's important to note that the commonly available DICOM medical imaging packages, often bundled with bespoke viewing programs for medico-legal purposes, may not be suitable for this purpose.
Editor Comment: "INNEG provide a bespoke viewer to our clients that allows the expert to review all imaging behind one easy-to-access GDPR-compliant share link. This is part of the complete record management package that we provide."
To support your cases effectively, our guide on How to Source High Calibre Expert Witnesses offers practical advice on selecting and instructing orthopaedic experts.
About the Author
Mr David L Shaw is a Consultant Orthopaedic Surgeon at Bradford Teaching Hospitals NHS Foundation Trust.
He became a Consultant in 1996 and has more than 25 years on-call trauma service. He continues to undertake trauma & fracture surgery as well as an active lower limb arthroplasty elective practice.
Mr Shaw started his medicolegal practice more than 25 years ago, and continues to advise on all aspects of orthopaedic surgery particularly lower limb arthroplasty & trauma. He is instructed by both Claimants and Defendants and can provide opinion on both clinical negligence and personal injury matters.
Mr Shaw can be contacted for all medico-legal work and to request his CV at info@inneg.co.uk
Tags:
- Orthotist Expert Witness
- Trauma
- Orthopaedic Expert Witness
- Orthopaedic Trauma
- Orthodontics Litigation
- Implant Misplacement
Expert Disciplines:
- Orthopaedic Surgery
About The Author

Mr. David L Shaw
Consultant Orthopaedic Surgeon
Mr. David L Shaw is a Consultant Orthopaedic Surgeon at Bradford Teaching Hospitals with over 25 years’ experience in trauma and lower limb arthroplasty. He has provided expert medico-legal opinions for more than 25 years, advising on clinical negligence and personal injury cases for both Claimants and Defendants.
For medico-legal enquiries or to request his CV, contact davidlshaw@inneg.co.uk.
From the Blog
Related Articles

Struggling to find the right expert? This guide shares practical tips and insider know-how to help clinical negligence solicitors secure reliable medico-legal support - faster and with less stress.

Understand why remote spinal assessments risk flawed medico-legal evidence - and why face-to-face exams are vital for defensible, accurate reports in spinal injury and negligence cases.

Understand how orthotic interventions shape spinal injury rehabilitation outcomes - essential for identifying overlooked care needs, building stronger claims, and maximising compensation accuracy.
Find out why 70+ legal firms partner with INNEG.
Request a callback, or contact us.
INNEG respects your privacy. Any information you share with us will be used only to respond to your query.
Phone
+44 161 870 2461Thank you for your request!
We will get back to you as soon as possible.