Acute Aortic Dissection: Medico-Legal Risks and Clinical Pitfalls
By Mr Donald Whitaker, Consultant Cardiothoracic Surgeon
Posted 17 February 2026
7 Minute Read

Acute aortic dissection is rare, rapidly fatal, and frequently misdiagnosed - making it one of the most high-risk and contested conditions in emergency medicine litigation.
The Definition
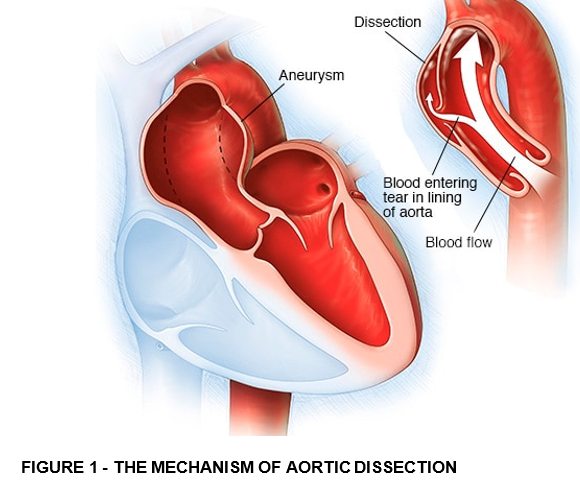
Acute aortic dissection is a sudden event in which blood from inside the aorta penetrates the innermost layer of the aortic wall (the intima) through a tear and enters the middle layer called the media. The blood then tears the media apart to create a true and a false lumen which is separated by a layer of media and intimal tissue. The outer layer will consist of adventitia and media and if this ruptures will usually lead to death of the patient.
Incidence
Acute aortic syndrome is defined as a group of related pathologies - aortic dissection, intramural haematoma and the complications arising from penetrating atherosclerotic aortic ulcer.
The conditions are linked together as a single syndrome because the treatment for all 3 is the same, when located in the ascending aorta, that is; emergency surgery.
Acute aortic dissection (AAD) is the commonest of the three entities, accounting for 95% of acute aortic syndromes.
Type A dissections involve the ascending aorta, according to the Stanford Classification. These are managed surgically by Cardiac surgeons whereas type B, involving the descending aorta are usually treated by vascular surgeons and can more often be managed conservatively.
Population-Based Study of Incidence and Outcome of Acute Aortic Dissection and Premorbid
Risk Factor Control 10-Year Results From the Oxford Vascular Study
Circulation. 2013;127:2031-2037 (Reference 1)
AAD usually presents as an emergency and as the incidence of acute aortic dissection is about 6 per 100,000 population per year, a typical Emergency Department which covers a population of 500,000 can therefore expect to see approximately 30 patients with acute type A aortic dissection per year.
Presentation
It is estimated that about 20% of patients with acute aortic dissection die before reaching medical care and a further 30% die before being able to be treated with emergency surgery in a cardiothoracic tertiary referral centre.
AAD can present with a variety of symptoms and signs and then particular tests are used to confirm or refute the diagnosis.
Symptoms
The typical presentation is with the symptom of sudden onset severe central chest pain (present in 95% of patients). Often this pain is described as "tearing" or "ripping" in nature and is also frequently described as the worse pain the patient has ever experienced. The pain may radiate to the back, neck arms, abdomen or legs.
In addition to the pain caused by the initial aortic tear, other symptoms and signs reflect ischaemia (reduction in blood supply) to organs such as the brain or spinal cord which may cause fainting, stroke and other neurological signs in the limbs. There may also be ischaemia of the heart causing ECG changes or a heart attack, ischaemia of the gut causing abdominal pain, nausea, vomiting and diarrhoea). The dissection may cause sudden leakage of the aortic valve and heart failure.
Fainting is present in 13% of patients presenting with AAD, elevated blood pressure in 28%, symptoms of stroke or focal neurological deficits in 17-42%, and a clinical picture of acute abdomen in 6%.
One can thus see that the symptoms and signs of AAD may clinically overlap with other, more common, clinical syndromes. For example, central chest pain is more commonly due to myocardial ischaemia as stand-alone heart attacks are more common than AAD or AAD with associated myocardial ischaemia. Additionally, AAD as a cause for an acute abdomen would be near the bottom of most general physicians' (or general surgeons' or ED staff’s) list of differential diagnoses for acute abdomen.
To put AAD in context, a typical Emergency department will receive hundreds of patients per year with heart attacks and acute abdomens but fare fewer AADs per year.
The relative rarity of AAD and its overlapping presentation with other more common conditions explains why patients with AAD are often missed diagnosed or the diagnosis delayed or missed altogether. When cases are missed, an ED expert is required to determine whether this was reasonable or a breach of duty.
Signs
A difference in the systolic blood pressure between the right and left arms is a well-known sign of AAD. However, a systolic blood pressure difference of greater than 20 mmHg is present in only 30% of AADs but a pressure difference between the arms of greater than 10mmHg is present in about 50% of the normal population. Thus the presence or absence of this sign has low sensitivity or specificity and in practice has little benefit.
Testing
Blood tests such as troponin and D-dimer may be raised but they are also raised in many other conditions and are thus not specific for AAD. ECG and CXR often show abnormalities but may be normal in a significant proportion of patients with AAD. Studies have shown that up to 30% of patients with AAD can have a normal ECG and 20% of patients with AAD do not have typical widening of the mediastinum on a CXR.
It is a contrast CT aortogram that is essential to make a definite diagnosis and refer to the patient for emergency cardiac surgery. Contrast CT aortogram is the most sensitive and specific and widely available test for AAD and is reported to have a 98% specificity. As with most clinical investigations, it is not 100% specific or sensitive.
Management
The mortality of patients with an acute aortic dissection is 1-2% per hour and this is why it is treated as a surgical emergency. Once definitively diagnosed at CT, surgery should be organised as soon as possible. Without surgery, the vast majority of patients with an acute type A aortic dissection will die.
Of those patients who survive to have a surgical repair of the dissection, the 30-day surgical mortality is 15-20%. Thus if patients survive to surgery they will on balance of probabilities survive.
Surgery
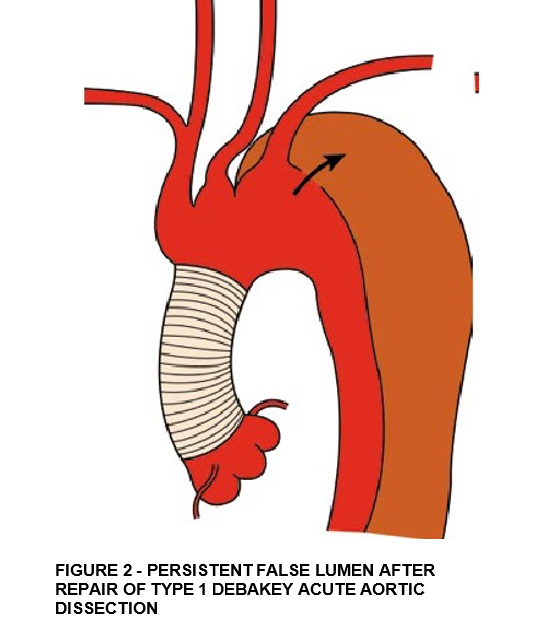
The purpose of surgery to treat type A aortic dissection is to replace the dissected portion of the ascending aorta containing the intimal tear to prevent rupture or cardiac tamponade. Sometimes it is only necessary to replace the ascending aorta with an interposition graft (Figure 2).
If the dissection has extended proximally to the aortic root or if the aortic root is aneurysmal then the aortic root will also need to be replaced. A damaged leaking aortic valve will need to be replaced or repaired and if the aortic root is being replaced then it would be necessary to replace the aortic valve at the same time.
Finally, when a patient has a DeBakey type 1 acute aortic dissection which involves both the ascending and the descending aorta, replacement of the ascending aorta, which is the lifesaving treatment, does leave the patient with a residual false lumen of the aortic arch and descending aorta (as shown in Figure 2). This persistent false lumen can become aneurysmal itself and will thus need lifelong monitoring with annual CT scans.
Timings and Causation with Missed or Delayed AAD
Timing for referral and transfer for emergency surgery is a frequently asked medicolegal question in determining causation in missed type A aortic dissection cases. That is - what is a reasonable time in which surgery should be organised? Unless patients present directly to a tertiary referral centre that contains a cardiac surgical unit, they will need referral to and transfer by emergency ambulance to such a unit. There is little published data, as far as I am aware, for average referral and transfer times which can make it difficult to support a logical opinion on what is a reasonable time in which surgery should be organised.
In an attempt to provide an answer, I conducted an audit looking at such timings. This audit analysed 20 consecutive patients referred for emergency type A dissection surgery over a one year period. The times were as follows with ranges given in brackets.
- Time from ED presentation to CT - 218 minutes (49-949)
- Time from CT to Referral - 99 minutes (17-290)
- Time from Referral to Transfer - 59 minutes (30-160)
- Time from Transfer to Arrival - 75 minutes (36-152)
- Time from Arrival to start for Surgery - 97 minutes (27-334)
Although there was a wide range of times, this represented a mean of 451 minutes (7 hours 30 mins) from ED presentation to arrival at accepting hospital of and a mean of 548 minutes (9 hours 8 minutes) from ED presentation to start for Surgery. This data can justify an opinion that it would be reasonable to expect most patients to have surgery within 9 hours and 8 minutes of presentation to the ED but also that in reality it can be much quicker or take far longer.
Interestingly a paper published recently which similarly analysed 334 patients in the UK found delays in diagnosis and transfers in 158 (47.3%) patients, fifty-two patients (15.6%) had an initial misdiagnosis and the condition of 56 patients (16.8%) deteriorated clinically before arrival in the operating theatre. Most significantly this study found that median time between arrival in the emergency department and the start of surgery was 9.5 hours which was very similar to my audit.
Time critical diagnoses and transfers of patients with acute type A aortic dissection in the UK: national audit of current practice
Anaesthesia 2025, 80, 248–258 (Reference 2)
6 Other Questions Frequently Asked in Aortic Dissection Cases
What would have been the likely recovery period?
Emergency surgery for acute aortic dissection invariably involves a median sternotomy (cut through the sternum). The usual, expected time for recovery from this type of operation would be 3 to 6 months. For a relatively young patient who was previously fit and well, I would expect the recovery period to be closer to 3 months than 6 months.
Would they have made a full recovery?
Yes, on the balance of probabilities they would make a full recovery.
What would be the likely prognosis?
After a recovery period of 3 to 6 months, the patient would make a full recovery and would have been able to partake in almost all normal activities. They would be advised to avoid isometric exercises (such as weight lifting) that can cause sudden increases in blood pressure.
Would they have needed to be reviewed throughout life?
Yes, on the balance of probabilities, they would be left with a residual aortic dissection of the descending thoracic aorta which would require annual life long monitoring with imaging (CT scan or MRI scan).
On a balance of probabilities, would they needed further intervention on the aorta during their lifetime?
It is well documented that the lifetime risk of requiring further aortic intervention following emergency repair of aortic dissection, although sometimes necessary, is less than 50% and so on the balance of probabilities the Deceased would not have required further intervention on his aorta.
Would life expectancy have been reduced as a result?
The question of life expectancy following repair of a type A dissection is quite a complex issue as there is conflicting data in the medical literature. The possible reason why the data varies in the medical literature includes publication bias as centres that have good results are more likely to attempt to publish their results. Also, the various studies are conducted over varying time periods on differing populations using differing surgical techniques and differing follow-up rates.
In my view, one has to be a little circumspect about applying data from case series in the literature to an individual case. However most studies suggest that the average mortality after repair of a type A dissection is about 5% per year and that the median survival is close to 10 years.
The most recent data published, and the data which I consider to be most relevant suggests that the life expectancy is about 10 years.
Below is a more detailed analysis of the long-term survival post type A aortic dissection repair:
Reference 3 - Long-term Follow-up of Patients with Acute Aortic Syndromes: Relevance of both Aortic and Non-aortic Events. Eur J Vasc Endovasc Surg (2018) 56, 200-208. (Corsini et al).
This is a single-centre retrospective observational study and included consecutive patients diagnosed with acute aortic syndrome and discharged between 2000 and 2016. It included 242 surgically treated type A aortic dissections. Long-term all-cause mortality was 5.4 per 100 patients per year in surgically treated type A acute aortic syndrome patients. This would suggest an approximate 50% mortality at 10 years.
Reference 4 - Outcomes after surgery for acute type A aortic dissection in ‘‘non-Marfan syndrome’’ patients with long life expectancy: A 24-year follow-up. Archives of Cardiovascular Disease (2017) 110, 14—25. (Piccardo et al).
This was a smaller study of only 66 patients. In the patients who had an interposition graft 10- year survival was 75%.
Reference 5 - Surgical management and long-term outcomes for acute ascending aortic dissection. J Thorac Cardiovasc Surg 2009;138:1349-57. (Stevens et al).
195 consecutive patients were studied and at 1, 5, 10, and 20 years postoperatively, survival was 84%, 69%, 55%, and 30%. This suggests that the median 50% survival is closer to 10 years than 20.
Reference 6 - Survival and reoperation in acute aortic syndromes—a single-centre experience of 912 patients. European Journal of Cardio-Thoracic Surgery 2023, 64(5)
This study analysed 494 patients with type A acute aortic dissection. It was found that 1, 5 and 10 year survival was 74.2%, 62.2% and 45.5% in Type A aortic dissection with no differences among treatment strategies. This paper with the largest group of patients studies therefore suggests that median survival is slightly less than 10 years.
Reference 7 - Survival following acute type A aortic dissection: a multicenter study. J Thorac Dis 2023;15(12):6604-6622
A total of 601 patients who had type A aortic dissection repair at several centres found that overall survival was 73.3% after the first year, 68.2% at 5 years, and 53.5% at 10 years. This robust study, therefore, also suggests that about half the patients can be expected to survive for about 10 years.
Tags:
- Aortic Dissection
- Breach of Duty
- Cardiac Negligence
- Expert Instruction
- Cardiology Expert Witness
About The Author

Mr Donald Whitaker
Consultant Cardiothoracic Surgeon
Mr Donald Whitaker is a Consultant Cardiothoracic Surgeon at King’s College Hospital NHS Foundation Trust, specialising in adult cardiac and thoracic surgery. He has particular expertise in acute aortic pathology, minimally invasive thoracic techniques, and complex cardiothoracic surgical care.
From the Blog
Related Articles
Essential reading for solicitors handling CHD claims - uncover key risks, missed follow-ups, and medico-legal pitfalls in adult congenital heart disease, with expert insight into real case examples.

Stroke care has transformed in recent years - but as cases rise, so do medicolegal dilemmas. Dr Kadam explores modern stroke treatment, key challenges, and the vital role of multidisciplinary teams.

Understand the risks and legal nuances of nasogastric tube complications to strengthen your clinical negligence claims and protect clients from preventable medical harm.
Find out why 70+ legal firms partner with INNEG.
Request a callback, or contact us.
INNEG respects your privacy. Any information you share with us will be used only to respond to your query.
Phone
+44 161 870 2461Thank you for your request!
We will get back to you as soon as possible.