Stroke Awareness Month: The Evolution of Stroke Care and the Medicolegal Dilemmas
By Dr Mustafa Kadam, Consultant in Acute, General and Stroke Medicine
Posted 05 May 2025
9 Minute Read

The burden of stroke is real and it is ever increasing. The number of patients experiencing a stroke has risen by 28% in the last 2 decades, to approximately 100,000 cases annually, and this is expected to continue to rise in the coming decade. No longer is it a disease of the older population, with epidemiological data now showing that nearly a quarter of patients experiencing a stroke are under the age of 65. Stroke care has significantly evolved over the last decade from improving hyperacute treatment strategies such as mechanical thrombectomy to an enhanced focus on stroke prevention and long term rehabilitation.
Stroke and Transient Ischaemic Attacks (TIAs) are time-sensitive neurological emergencies and any delay or lapses in care can have devastating outcomes.
This article will touch on the key areas of understanding stroke and TIAs together with the multidisciplinary team involved in the management of these conditions. I will then delve into the medicolegal dilemmas of stroke care from my perspective as an expert witness in this area.
Understanding Stroke and TIA
Ischaemic Stroke
Almost 84% of all strokes are ischaemic strokes. This is when a blood clot obstructs an artery in the brain reducing the flow of blood to that part of the brain it supplies blood to. The severity of ischaemic stroke depends on the type of the artery affected, how quickly this is recognised and managed and finally the area of the brain that has been damaged. The artery can be a large vessel, medium vessel or a small vessel.
Time-sensitive reperfusion interventions are crucial and include thrombolysis (dissolving the clot with intravenous medications) or mechanical thrombectomy (the process of actually extracting the blood clot if it is occluding a large vessel).
The recent National Clinical Guidelines for Stroke have emphasised a shift from the previously strict 4.5 hour “treatment window” to being more inclusive for patients who may have a favourable “core-perfusion” mismatch on advanced imaging. This means that if patients present with an unknown onset time or have woken up with stroke symptoms, they could still be eligible for these hyperacute interventions if they have enough salvageable brain tissue (the penumbra) in comparison to the areas of the brain that have been permanently damaged (the core) as a result of the stroke.
Further management of ischaemic strokes include to investigate for the underlying cause through a detailed work-up and rehabilitation in hospital or in the community through Early Supported Discharge (ESD).
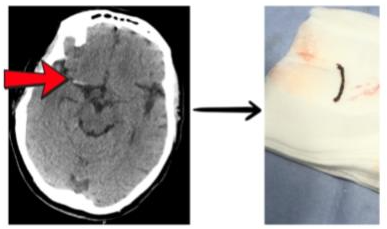
Figure 1 demonstrates a CT scan of a patient who presented with dense left sided face, arm and leg weakness as a result of a blood clot within the right middle cerebral artery. The patient rapidly recovered as soon as her blood clot was removed with mechanical thrombectomy.
Haemorrhagic Stroke
Haemorrhagic strokes occur when there is bleeding in the brain caused by a weakened blood vessel. There could be several causes including hypertension, ruptured aneurysms, use of ‘blood thinners’ (anticoagulants), underlying brain lesions or impaired blood vessel wall integrity due to conditions such as cerebral amyloid angiopathy. The management would be to correct or reverse any oral anticoagulant drugs in the system (if appropriate), aggressively manage blood pressure and investigate for any other underlying causes such as those detailed above. Some patients may also require urgent neurosurgical intervention.
Transient Ischaemic Attacks (TIAs)
Also referred to as a “mini-stroke”, TIA’s cause temporary neurological symptoms (resolving within 24 hours, although often much sooner) which could be a critical warning of an impending ischaemic stroke. Approximately 6-7% of patients will have experienced a stroke within 1 week following an episode of a TIA without appropriate preventative measures being put in place.
Patients who experience a suspected TIA should be urgently seen in a dedicated neurovascular service where they have a detailed assessment completed by stroke specialists. The assessment begins with actually making the diagnosis of TIA and this can be challenging in clinical practice due to number of “mimics” that are also seen in such services.
Following a diagnosis of a TIA, clinicians initiate patients on antithrombotic treatment (antiplatelets or anticoagulants where appropriate) together with risk factor reduction strategies to help manage blood pressure, cholesterol, diet, diabetes, exercise and smoking. Further investigations are also considered and could include, where appropriate; blood tests, electrocardiograms, brain imaging, carotid imaging and assessment of the heart.
Multi-disciplinary Team (MDT) Approach
There are several disciplines involved in the management of patients presenting with acute stroke. Each has an equally important role in ensuring the best outcomes for our patients.
The disciplines involved include:
- 111 Or 999 Call Operators - trained in recognising if a patient is experiencing a stroke in order to ensure appropriate help is obtained in a timely manner.
- Paramedics - stabilising patients and ensuring timely and appropriate conveyance to a stroke centre with the appropriate facilities in managing hyper-acute stroke patients. It should be noted that patients may require conveyance to a comprehensive stroke centre if mechanical thrombectomy is not delivered at the initial site. This is standard of care in some areas.
- A&E physicians and GPs - recognising and diagnosing patients presenting with acute stroke or TIA if they did not present via ambulance.
- Stroke Consultants and Specialist Registrars, Advanced Nurse Practitioners and Nurse Consultants - for the diagnosis, investigation and management of patients presenting with acute stroke including delivery of thrombolysis and recognising when patients need referral for mechanical thrombectomy.
- Neuroradiologists - for reviewing and reporting brain imaging.
- Interventional Neuroradiologists - for undertaking mechanical thrombectomy.
- Neurosurgeons - for when patients presenting with stroke may require urgent neurosurgical intervention, particularly in the context of haemorrhage or when a decompressive hemicraniectomy may be required for patients presenting with very large strokes.
- Stroke Nurses - within a dedicated stroke unit, trained in recognising complications following a stroke and careful observation of patients.
- Allied Health Professionals - including physiotherapists, occupational therapists, speech and language therapists, dieticians and psychologists - all involved in the rehabilitation of patients following their stroke.
Medicolegal Dilemmas in Stroke
Here are some insights on the types of cases I have had to opine on when it comes to the management of patients experiencing an acute stroke or TIA.
1. Stroke Prevention
This can be further broken down into “primary” and “secondary” prevention.
The goal of primary prevention in stroke is to prevent it from ever occurring in the first place. This requires robust attention into managing certain risk factors such as hypertension, atrial fibrillation, hypercholesterolaemia, diabetes, diet or smoking and alcohol consumption. Whilst of course, some of these risk factors are dependent on the patient’s choices, there are certain cases when a breach of duty may occur. For instance, in the case of a patient who had been identified to be hypertensive, but no measures were put in place to control their blood pressure prior to them developing a hypertensive haemorrhagic stroke. Another example would be where the patient who was known to have atrial fibrillation with associated significant risk of developing a cardioembolic stroke however no measures were put in place to commence them on oral anticoagulants.
Secondary prevention in stroke focuses on early detection of the condition and putting in measures to prevent further worsening or recurrence. In the context of a TIA for instance, patients must be referred to a neurovascular service whereby a detailed assessment (as described above) should be undertaken and steps implemented to reduce the risk of stroke recurrence. Failure to do so constitutes a breach of duty and puts the patient at a significant risk of a stroke.
2. Delayed Or Misdiagnosis of Stroke/TIA
There needs to be a high index of suspicion for stroke whenever a patient develops acute onset focal neurological deficits however there are times when the patient does not have the typical deficits as advertised in the FAST scheme (Facial weakness, Arm weakness, Slurring of speech and Time to call for help). This creates a dilemma for healthcare professionals, particularly if patients have non-specific symptoms. Nonetheless, a detailed history and clinical examination is mandated like with all things in medicine and the question here is “whether the clinician’s management of the patient could be supported by a reasonable body of clinical opinion”
3. Inadequate Acute Stroke Treatment
This area relates to whether the treatment afforded to the patient when they presented acutely was at the standard of care expected for them including whether they were eligible for thrombolysis or thrombectomy. Independent experts are critical in assessing what should have been done including a close look at the timings of the onset of stroke and their time of presenting to hospital. Based on the patient’s symptoms and neuroimaging, conclusions could be drawn on the what the available treatment strategies could have been considered for the patient together with answering the question on “whether the outcome would have been better but for the lapses in care”
Conclusion
Ultimately, stroke management requires an MDT approach, and all components of the MDT are critical in ensuring the best outcomes for our patients.
About the Author
Dr Mustafa Kadam is a triple accredited Consultant Physician in Acute Internal Medicine, General Internal Medicine and Stroke Medicine at Guy’s and St Thomas’ NHS Foundation Trust (GSTT).
In his day-to-day clinical practice, he manages medical patients acutely admitted to hospital with a wide array of medical presentations. He interfaces directly with colleagues from within the Emergency Department and the London Ambulance Service. He also manages patients through the Same Day Emergency Care (SDEC) services.
In addition, he is on the Thrombolysis / Thrombectomy (HASU) on-call rota at St George’s University Hospital NHS Foundation Trust, and he also runs a weekly TIA / Neurovascular clinic at GSTT.
He is a Medical Information Officer at his Trust and is also the South London Regional Adviser for the Royal College of Physicians (RCP).
To request his CV or for any medico-legal matters, he can be reached at mkadam@ardentsupport.uk
Tags:
- Misdiagnosed Stroke
- Stroke Claims
- Stroke Misattribution
- Brain Trauma
- Neurosurgery
Expert Disciplines:
- Stroke Medicine
About The Author
Dr Mustafa Kadam
Consultant in Acute, General and Stroke Medicine
Dr Mustafa Kadam is a Consultant in Acute, General and Stroke Medicine at GSTT. He also works at St George’s, runs a TIA clinic, advises the RCP, and supports emergency and same-day care services.
From the Blog
Related Articles

Understand perinatal stroke’s complex impact and medico-legal challenges to strengthen clinical negligence claims involving newborn brain injury through expert multi-specialty insights and evidence.

Ensure expert alignment with injury type - this guide helps solicitors navigate specialty overlaps in spinal and brain cases, reducing risk of flawed instruction and improving report credibility.

Gain expert insights on neurosurgical clinical negligence, MDT challenges, and evidence essentials to strengthen your cases and navigate complex claims with confidence and precision.
Find out why 70+ legal firms partner with INNEG.
Request a callback, or contact us.
INNEG respects your privacy. Any information you share with us will be used only to respond to your query.
Phone
+44 161 870 2461Thank you for your request!
We will get back to you as soon as possible.