The Complications of Cholecystectomy
By Professor Poston, Consultant General Surgeon
Posted 20 August 2026
7 Minute Read

Cholecystectomy may be a common abdominal operation, but when bile duct injury occurs, the key medico-legal question is whether this was a recognised complication or evidence of substandard surgical care.
Cholecystectomy (surgical removal of the gallbladder under general anaesthetic, usually for symptomatic gallstones and their complications) is one of the most frequently performed abdominal operations both in the NHS and private sector. The usual indication for cholecystectomy (see NICE guidance cg188 2014) is symptomatic gallstones in the gallbladder causing recurrent biliary colic (gallbladder pain). The general surgical consensus is that asymptomatic gallstones found incidentally in the investigation of other symptoms don’t warrant surgery and should be safely left alone. However, symptomatic gallstones can cause life threatening complications if they migrate out of the gallbladder into the bile duct between the liver and bowel (see figure 1 showing the usual anatomy of the gallbladder and bile ducts, seen in 50% of people), causing cholangiolithiasis (infected obstructive jaundice due to bile duct obstruction) and acute gallstone pancreatitis, both of which warrant urgent surgical intervention. Furthermore, while thankfully uncommon, but usually incurable, symptomatic gallstones can cause gallbladder cancer.
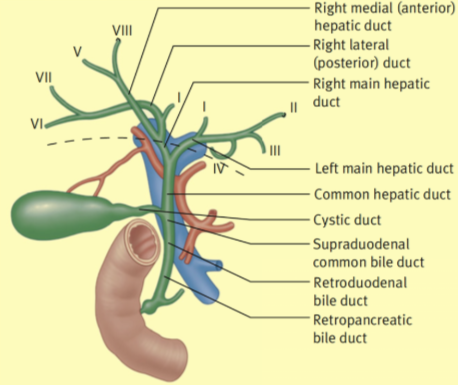
Figure 1. The usual anatomy of the gallbladder and bile ducts, seen in 50% of people.
Complications of cholecystectomy include those of surgery under general anaesthesia (heart attack, deep vein thrombosis and pulmonary embolism, chest infection) and those of abdominal surgery in general (wound infection, wound breakdown and dehiscence, urinary tract infection, incisional hernia) and these complications would be widely regarded as well-recognised and non-negligent. Complications specific to cholecystectomy include postoperative bile leak which usually occurs from a duct of Luschka, a bile duct running in the gallbladder fossa bed of the liver, closely attached to the gallbladder which may be inadvertently bruised and subsequently leaks bile in the postoperative period into the patient’s abdomen, or a leak from the cystic duct stump (previously connecting the gallbladder to the bile duct) if the clip placed to seal the cystic duct fails in the postoperative period, again causing a bile leak into the abdomen and bile peritonitis. There is a substantive body of responsible General Surgeons who reasonably regard these complications a well-recognised and non-negligent.
From a medico-legal perspective, it is important to distinguish between a recognised complication and a complication that may indicate substandard care. The mere fact that a patient develops a post-operative complication following cholecystectomy does not automatically imply negligence. Solicitors will usually need to consider whether the complication was a recognised risk, whether it was appropriately consented for, whether reasonable steps were taken to minimise that risk, and whether the complication was recognised and managed appropriately once it occurred.
The most serious complication of cholecystectomy, whether performed laparoscopically (keyhole surgery), which are the majority of cases, or by the traditional open route (usually following conversion from laparoscopic surgery for concerns regarding operative difficulty and safety) is injury to the bile duct (either the upper hepatic ducts or lower common bile duct, see Figure 1). This can occur for a number of reasons. Firstly, the surgeon gets lost, frequently when the severity of gallbladder inflammation (cholecystitis) is so bad that the gallbladder fuses to the bile duct with scar tissue, which the surgeon then fails to appreciate. The surgeon then mistakes the bile duct for the cystic duct, so operating to the left side of the bile duct which is then clipped and divided in the mistaken belief that they are dividing the cystic duct to free the gallbladder. The second cause of iatrogenic (doctor caused) bile duct injury is trying to disconnect a gallbladder that is fused to the bile duct by chronic inflammation and scar tissue, from the bile duct and in so doing, damaging the bile duct. A third cause of bile duct injury during cholecystectomy is inappropriate use of diathermy cautery to dissect the gallbladder away from the liver and bile duct, using excessive cautery power, operating too close to the bile duct or a combination of both. Such bile duct injuries are generally considered negligent and indefensible.
Steps that a surgeon should take to avoid iatrogenic bile duct injury include firstly abandoning the procedure and referring to patient to a specialist Hepatobiliary surgeon. Second, converting to open surgery to improve safe access. Third, consider performing a subtotal cholecystectomy, removing all the gallstones from the gallbladder but leaving a cuff of gallbladder against the bile duct. Lastly, in very elderly patients, performing a cholecystostomy, opening the gallbladder and removing the gallstones before leaving the gallbladder in situ. Steps to reduce the risk of bile duct injury included performing an operative cholangiogram (an Xray examination of the gallbladder and bile ducts during the cholecystectomy operation) to confirm the biliary anatomy and relationship of the gallbladder to the bile duct system and performing the ‘critical view of safety’, first described by Strasberg over thirty years ago (see Figure 2). The purpose of the critical view of safety is to establish the anatomy of Calot’s triangle, the potential space between the cystic duct, common hepatic duct and cystic artery (blood supply to the gallbladder), see Figure 1. If this space can be clearly defined and the surgeon confirms that there are only two tubular structures crossing this operative field (the cystic duct and cystic artery), then if the surgeon is totally satisfied and takes photographic evidence (ideally by video, saved in the patient’s electronic case record), then the cystic duct and artery can be safely clipped and divided in order to release the gallbladder. Such practice has been the standard of care in the Netherlands since 2010 and has led to a near 75% reduction in iatrogenic bile duct injuries at laparoscopic cholecystectomy.
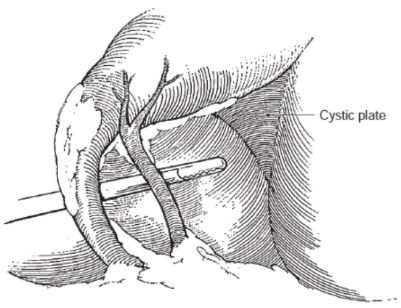
Figure 2. The dissection required to demonstrate the ‘critical view of safety’. Calot’s triangle is dissected free of all tissue until only the cystic artery and cystic duct connecting the gallbladder to the common hepatic duct to form the common bile duct (see Figure 1) are the only structures in the operative field.
For solicitors reviewing a potential bile duct injury claim, the operation note is often central. Key questions include whether the surgeon documented the operative findings, whether Calot’s triangle was safely dissected, whether the critical view of safety was achieved, whether an intraoperative cholangiogram was considered or performed, and whether any difficulty due to inflammation, scarring or abnormal anatomy was recognised. Where the anatomy was unclear, the records should explain what steps were taken to reduce risk, such as conversion to open surgery, subtotal cholecystectomy, cholecystostomy, or referral to a specialist hepatobiliary surgeon.
Roughly 50% of iatrogenic bile duct injuries are identified or suspected during the index cholecystectomy, but unfortunately, 50% are not identified at the time they are caused. If identified, then these patients are transferred on a blue light to the regional Hepatobiliary surgery centre for bile duct reconstruction surgery (hepaticojejunostomy Roux-en-Y). Those in whom the bile duct injury is neither suspected or identified are usually sent home later that same day, becoming increasing unwell at home with jaundice and bile peritonitis before being returned to hospital as an emergency readmission. Any patients returning to hospital in such circumstances must be considered an iatrogenic bile duct injury until proven otherwise (a bile leak from a duct of Luschka or the cystic duct), and if so, then transferred urgently to the designated regional centre for Hepatobiliary surgery.
Post-operative management is also relevant. If a patient becomes increasingly unwell after discharge, with symptoms such as abdominal pain, jaundice, fever, sepsis or signs of bile peritonitis, clinicians should have a high index of suspicion for bile leak or bile duct injury. In a medico-legal claim, solicitors may need to examine the timing of deterioration, the investigations performed, whether imaging was arranged promptly, whether senior surgical input was obtained, and whether referral to a regional hepatobiliary centre was made without avoidable delay.
In my experience both repairing iatrogenic bile duct injuries caused by other surgeons and preparing breach of duty reports to the Court on iatrogenic bile duct injury claims, there is frequently no contemporaneous documented evidence that the surgeon has taken any such steps to reduce or avoid the risk of iatrogenic bile duct injury or has simply got lost, not considering the bale-out options (above) to reduce the risk of bile duct injury. In my opinion, iatrogenic bile duct injury in such circumstances is indefensible and the settlement not inconsiderable, bearing in mind the potential lifetime risks of serious life-threatening complications, including chronic recurrent cholangitis, secondary biliary cirrhosis and possible liver transplant.
Tags:
- Cholecystectomy
- Debulking Surgery
- Jaundice
Expert Disciplines:
- General Surgery
About The Author

Professor Poston
Consultant General Surgeon
Professor Poston recently retired from full-time NHS clinical practice as a consultant General Surgeon, but continues to work part-time for the NHS in an administrative capacity. He enjoys an international reputation in Hepatobiliary (liver and bile duct) surgery, on which he has published extensively. He has provided over 3,000 reports on allegations of breach of duty in abdominal surgery (both elective and emergency) to the Courts in England, Wales, Scotland, Northern Ireland, Ireland, Hong Kong, the Cayman Islands, St Helena and the USA for over 30 years, roughly 70% claimant instructed. He remains fully registered on the GMC's Specialist Register
From the Blog
Related Articles

Gain crucial insights on complex consent and surgical risks in paediatric spinal cases to strengthen your clinical negligence claims and better support vulnerable patients and their families.

For solicitors reviewing potential paediatric bone and joint infection claims, the focus is rarely just whether antibiotics were given. The more important questions are whether infection was considered early enough, whether imaging and microbiological investigations were adequate, whether surgery addressed the true extent of disease, and whether follow-up accounted for growth, function and long-term harm.

Pressure ulcers often become legal fault lines - this blog examines how prevention, documentation, and evidence determine liability, defensibility, and outcomes in clinical negligence claims.
Find out why 70+ legal firms partner with INNEG.
Request a callback, or contact us.
INNEG respects your privacy. Any information you share with us will be used only to respond to your query.
Phone
+44 161 870 2461Thank you for your request!
We will get back to you as soon as possible.