Medicolegal Assessment of Spinal Infection: Diagnosis, Treatment, Outcome and a Medicolegal Experience.
By Mr N V Todd , Consultant Neurosurgeon & Spinal Surgeon
Posted 28 May 2025
11 Minute Read

Spot spinal infection claims early with expert insights - improve outcomes, reduce risk, and maximise claim value by understanding key diagnostic and treatment failures.
Spinal infection is an uncommon pathology clinically but it is potentially devastating. It is over-represented in clinical negligence litigation because delayed diagnosis and treatment of spinal infection is common and often causes severe, irreversible neurological deficits. Functional deficits and quantum can be considerable. Excellent outcomes are expected where there has been early diagnosis and treatment of spinal infection particularly before there are significant neurological deficits. By contrast if motor weakness is present at the time of treatment 90% have long-term weakness.
Sites of spinal infection
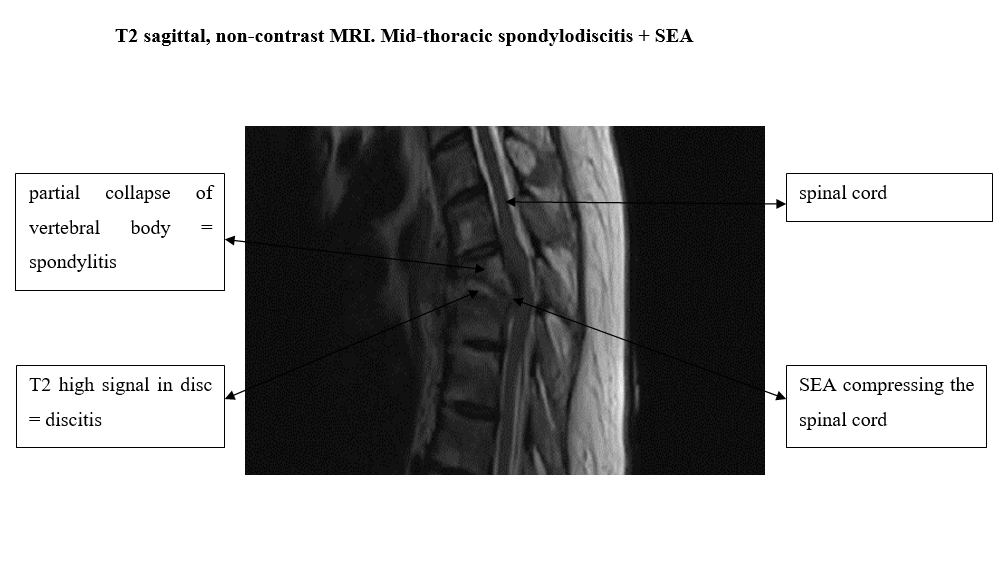
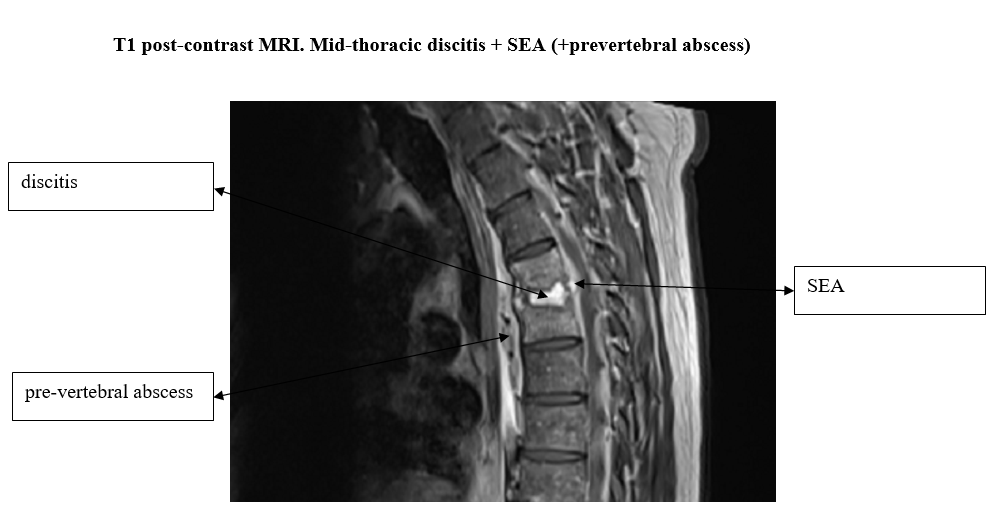
The anatomical site(s) of spinal infection include (i) the intervertebral disc (discitis) (ii) a vertebral body (spondylitis) (iii) the epidural space or (iv) around the spine (paravertebrally). Frequently there is infection in more than one compartment, infection of a disc and an adjacent vertebral body is common (spondylodiscitis). Spinal infection can occur at any level in the spine: it affects the cervical spine in about 10% of cases, thoracic spine in 30% of cases, lumbar spine in 60% of cases. Multiple levels are affected in 10-15% of pyogenic infections. Intradural infection, subdural or intramedullary abscesses, are well-recognised; they are rare and will not be further considered here.
Sources of Infection
Spinal infection can be caused by direct inoculation of micro-organisms into the spine for example from a surgical procedure, a spinal injection (for pain management), placing an epidural catheter or stabbing. It can be from an adjacent source of infection such as a diverticular abscess. The commonest cause is haematogenous spread from a peripheral source of infection. There is infection in another part of the body, micro-organisms circulate in the blood (bacteraemia) and they settle in the spine where they proliferate. Commonly the peripheral infection is minimally symptomatic and the patient is unaware of it. The incidence of spinal infection is approximately 1-2/10,000 hospital admissions. The incidence of spinal infection is rising because the incidence of predisposing systemic conditions such as diabetes mellitus, intravenous (IV) drug abuse and alcoholism are rising.
Infecting organisms
Many micro-organisms are capable of causing spinal infection. Internationally a common cause is Mycobacterium tuberculosis (TB). In the UK infection is usually pyogenic, Staphylococcus aureus is the most common organism found in about two-thirds of cases (methicillin-resistant Staph aureus is increasingly prevalent). No causative organism is identified in up to 40% of patients (despite extensive attempts to culture an organism).
Diagnosis
The symptoms and signs are non-specific, a high index of suspicion is needed. The common signs and symptoms are spinal pain (90%), radiating nerve root pain (50%), sensory disturbance (40%), motor weaknesses (50%), reduced tendon reflexes (35%) and/or fever (68%) (Table 1). Previously a diagnostic triad of fever, spinal pain and neurological deficits was emphasised but this is only present in 8% of cases1. Ideally a history for risk factors should be identified (Table 2), one or more risk factors is found in 98% of cases1; unfortunately this is rarely assessed. Neck and low back pain are common, a severe exacerbation of pain is of concern. Thoracic pain is a potential red flag because degenerative spinal pain is less common in the thoracic spine, thoracic pain suggests a serious disorder (infection or cancer).
If the differential diagnosis includes spinal infection blood tests and imaging should be performed urgently. Inflammatory markers, white cell count (WCC) and C-reactive protein (CRP) are typically elevated, the CRP is elevated in 90% of cases2. Blood cultures should be performed; they are positive in about 50%3. MR imaging pre- and post-contrast is the gold standard with sensitivity and specificities of over 90%. CT imaging is not used for primary diagnosis, it is useful to evaluate the bony pathology and/or for biopsy.
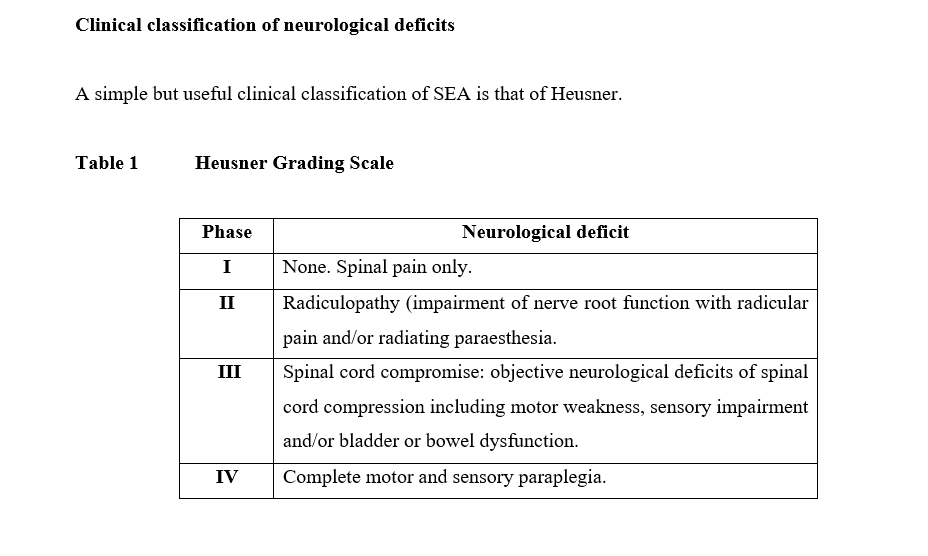
Phase 1 is localised spinal infection which can be within the epidural space itself, within a vertebral body or within an intervertebral disc. Typically there is fever, there is typically an elevated CRP; the white cell count may only be modestly elevated in the early stages. There is no neurological deficit.
Phase 2 is the development of a radiculopathy (impairment of nerve root function) with radicular pain and/or radiating paraesthesia (together with the evidence of infection noted above).
Phase 3 is the presence of objective neurological deficits of spinal cord compression including motor weakness, sensory impairment and/or bladder or bowel dysfunction.
Phase 4 is the development of a complete lesion (paralysis). Paralysis is an ominous development; few patients with paralysis recover sufficient motor function to enable the patient to walk.
Phases 1 to 3 can progress at rates that differ from patient to patient. In fulminant infection phases 1 to 3 might take only a few days. Once there are objective signs of spinal cord involvement and/or sensory disturbance (phase 3) paralysis can occur very rapidly (for example within a few hours).
Neurological deterioration (phases 3 and 4) in patients with SEA can be a consequence of (i) compression of the spinal cord from an SEA (ii) a consequence of spinal cord ischaemia which is caused by vascular thrombosis and/or (iii) spinal cord compression from spinal deformity.
Biopsy or not?
The ideal is isolation, and identification of the antibiotic sensitivities, of the infecting organism. Tissue biopsy is superior to blood cultures but a positive culture is only found in 50% of biopsies (perhaps because many are given antibiotics prior to biopsy). Whether to treat with antibiotics prior to a positive culture is controversial. In this author’s opinion if there is a known primary infection or positive blood cultures with a known and typical organism (such as Staph aureus) it can be assumed that that is cause of spinal infection and antibiotics can be started without a tissue biopsy. If there is no known organism, or the cultured organism is not plausible, a tissue biopsy should ideally be performed before antibiotics are given. An infected disc or vertebral body can be biopsied, via CT or biplanar X-ray guided approaches. If emergency surgery is required for spinal cord compression tissue is biopsied and antibiotics can then be given intraoperatively. If a biopsy is recommended prior to antibiotic treatment the concern is that this can take up to 2-3 days to be performed in District General Hospitals (DGHs). Clinicians must consider whether such a delay is safe? Where there is a focus of probable infection in one vertebral body with no neurological deficit and low inflammatory markers biopsy before antibiotics will often be the best course. I would be concerned about not treating with antibiotics where there is any neurological deficit as these patients can deteriorate rapidly to severe, irreversible spinal cord injury. If a decision is made to delay antibiotic treatment in such cases (and there is a range of opinion) it may be that that decision, even if supported by a reasonable body of clinical opinion, is illogical. Of course the ideal is to know the infecting organism and to treat that organism specifically but given that only 50% of tissue biopsies are positive and many patients are successfully treated with no known organism the Court would need to consider whether it is logical to expose patients to, potentially severe and irreversible neurological deterioration, by withholding antibiotics for, perhaps, several days.
Treatment
Treatment of spondylodiscitis with no SEA and no neurological deficit is primarily a combination of supportive clinical management and high-dose effective antibiotic therapy. Where the infecting organism has been cultured and antibiotic sensitivities obtained the infection can be treated with specific antibiotics. Where the organism, at that time, is unknown a broad-spectrum antibiotic plus an antibiotic with specific anti-Staphylococcal activity should be used initially. Antibiotics should be given in high doses, intravenously (IV) for at least 2 weeks, then orally for 6-8 weeks until infection is cured (patients should be monitored, see below). Low dose, oral or ineffective antibiotic treatment can suppress the systemic effects of infection such as reducing fever and the CRP can come down but spinal infection is not treated and recurs.
The surgical management of SEA is controversial, all SEA patients require antibiotic treatment as above. Surgical drainage of the SEA is mandated where there is a large SEA causing neurological deficits and/or spinal cord compression on MRI (unless there is a contraindication to surgery, see below). The precise nature of the surgical procedure and whether spinal instrumentation is needed is optimised on an individual patient basis. Antibiotic-alone treatment without surgery can be considered (i) in patients with severe comorbidities preventing surgery (ii) holocord abscesses where surgical drainage of the SEA may be unachievable (iii) early SEA with no neurological deficit and no radiological cord compression or (iv) complete motor and sensory paralysis >72 hrs where functional recovery is improbable. Meticulous monitoring is required. Antibiotic-alone treatment of SEA is associated with progressive neurological deficits in 6-49% of cases; put another way neurological deficits are 4x more likely to occur with antibiotic-alone treatment of SEA than surgery + antibiotics3.
Paraspinal abscesses commonly resolve with antibiotic treatment, probably because paraspinal abscesses are more vascularized than SEAs. If a large paraspinal abscess fails to resolve CT-guided aspiration can be considered. Spinal instrumentation is used where there is significant pre-operative deformity (typically caused by vertebral body collapse), where there is a risk of future deformity (after decompressive laminectomy for a posterior SEA with anterior vertebral body involvement) or in cases of late deformity (typically a late progressive kyphotic deformity).
Monitoring
All patients must be carefully monitored, clinically, haematologically and radiologically. Clinical monitoring of the neurological status is paramount. Neurological observation charts should be completed, initially 4-hourly. An ASIA chart should be completed daily. Any neurological deterioration mandates immediate reassessment. With effective treatment neurological deficits do not progress and spinal pain improves, serial CRPs fall, serial MRIs show resolution of infection over longer time-periods. Treatment-failure (increased neurological deficits or deformity, rising CRPs, progression of infection such as an enlarging SEA on MRI) is common. This mandates immediate review of treatment. Are the antibiotics appropriate to the infecting organism, are they being given in appropriate doses IV? Are further blood cultures or a tissue biopsy required. If infection is progressing should surgical debridement be performed, or repeated? Is there new or progressive deformity that requires surgical stabilisation?
Outcomes
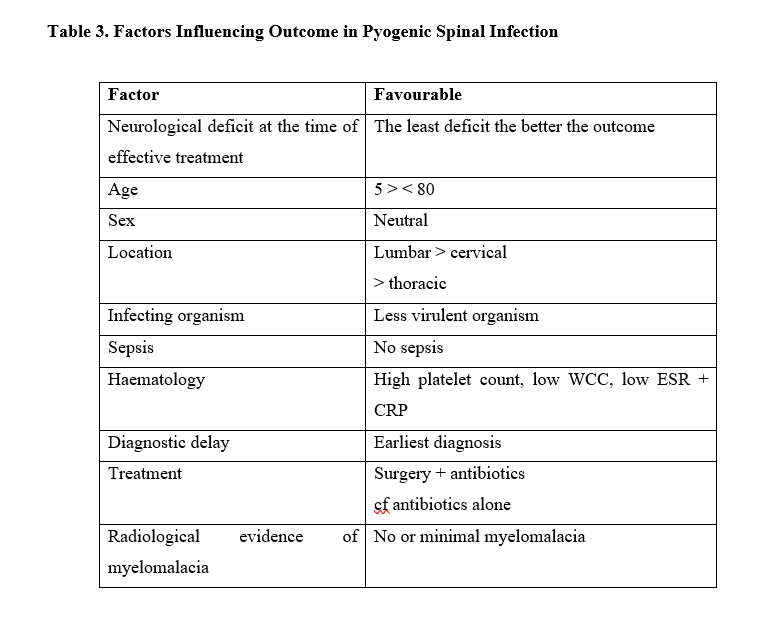
The long-term outcome in patients with a spinal infection is dependent upon a number of factors (Table 3). The most important factor is the patient’s neurological state at the time of definitive treatment. Other factors include age, location of infection, the infecting organism, whether sepsis is present or not, the results of haematological markers, whether there is diagnostic delay, the type of treatment and radiological evidence of myelomalacia (spinal cord damage) preoperatively. There are three predominant mechanisms that cause neurological deterioration in spinal infection. The first is compression of the spinal cord from the abscess. The second is an ischaemic myelopathy caused by thrombosis of blood vessels, particularly veins draining the spinal cord. The third potential mechanism is deformity causing spinal cord compression. Where the mechanism of injury is largely compression of the spinal cord and where there is a compressive spinal abscess decompression/drainage of the abscess relieves spinal cord compression and typically, with antibiotics, the neurological deficit stops progressing at that point. Where the neurological deficit is caused by vascular thrombosis the only treatment is antibiotics. With ideal treatment the rate of neurological deterioration is about 1%.
The most important determinant of outcome is the neurological deficit at the time of treatment. There is a marked trend to neurological improvement. In patients with neurological deficits at the time of treatment about 70% improve neurologically with good management. With negligent management patients commonly deteriorate neurologically. They can also improve with rehabilitation but, of course, they start from a lower base-line; many do not improve functionally.
Mistakes. A Medicolegal Experience.
The author has provided over 100 medicolegal reports in cases of spinal infection. The medicolegal cases set out below are taken from that medicolegal experience i.e. they are all “real” cases. All had avoidable, poor neurological outcomes.
Failed diagnosis, failure to act upon a differential diagnosis or failure to act upon advice. This is the commonest error. A 36 yr old IV drug abuser had thoracic spinal pain, fever and loss of lower limb sensation (4 red flags). He was discharged without investigation or treatment (negligent management). Another patient had a differential diagnosis that included “spinal discitis”. No blood tests or MRI were performed (negligent). In another case General Physicians were advised by a Spinal Surgeon was to arrange an urgent MRI to diagnose probable SEA, this advice was ignored (negligent). All 3 patients deteriorated with severe deficits.
Failure to act upon blood tests. This is also a common error. A patient with severe cervical pain but no neurological deficits had blood tests, the CRP was 165 mg/l (highly elevated, normal <10 mg/l). There are many causes of a raised CRP (it is a sensitive, not a specific test) but in context cervical spinal infection was the obvious diagnosis. The raised CRP was not acted upon and the patient was discharged (negligent). She was re-admitted 2 days later quadriplegic.
Failure to treat with appropriate antibiotics. A 32 yr old woman had a lumbar microdiscectomy for sciatica. There was a post-operative Staph aureus discitis. Low dose oral flucloxacillin (500 mg bd po) was given and continued for over 2 years (negligent). Serial MRIs showed progressive spondylodiscitis finally causing collapse of the L2/3, L3/4 and L4/5 vertebral bodies, with no neurological deficit. A decision was made to debride and reconstruct the spine anteriorly, the patients woke up paraplegic.
Failure to treat an SEA surgically and to monitor carefully A 56 yr old man presented with variable signs of myelopathy, 2 doctors recorded objective motor weakness, one did not. An MRI demonstrated an SEA centred at C3/4 causing cord compression radiologically. A Neurosurgeon decided to treat with antibiotics-alone (probable negligence, though arguable). The patient was discharged back to a DGH where he was not monitored (negligent). The patient was readmitted 6 days later quadriplegic, the SEA was decompressed via a C3/4 anterior cervical decompression (ACD), which was the ideal treatment initially. There was no functional recovery.
Failure to monitor (clinically, haematologically and/or radiologically). This is very common; it seems not to be understood that treatment failure is common. There are many cases where neurological deterioration occurs despite antibiotic treatment; neurological monitoring was not performed (negligent) until the patient the patient had severe deficits. A patient with spondylodiscitis was treated with antibiotics-alone. A rising CRP and white cell count (WCC) were ignored (negligent) until the patient deteriorated with an incomplete paraplegia. MR imaging demonstrated a new SEA compressing the cord. The SEA was drained but there was minimal improvement. A small group of patients have progressive deformity. A 70 yr old man had apparently successful treatment of C5/6 spondylodiscitis. He complained of a progressive chin-on-chest deformity. Serial X-rays showed a progressive cervical kyphotic deformity. No action was taken (negligent) until he had a severe incomplete paraplegia.
Despite best treatment with apparent cure of infection there can be late recurrence. A 25 yr old IV drug abuser had successful treatment of a C6/7 spondylodiscitis. After 2 weeks of IV and 8 weeks of oral antibiotics he was pain-free with no neurological deficits, the CRP was <5 mg/l (normal). Antibiotics were stopped and he was discharged. There was no warning that, uncommonly, there can be late recurrence of infection (negligent). There were progressive symptoms and neurological deterioration to an incomplete paraplegia.
Conclusion
The failure to diagnose and treat spinal infection is common. The typical consequence is neurological injury that in the great majority of patients was avoidable. Quantum is typically large where negligent management has caused incomplete or complete paraplegia.
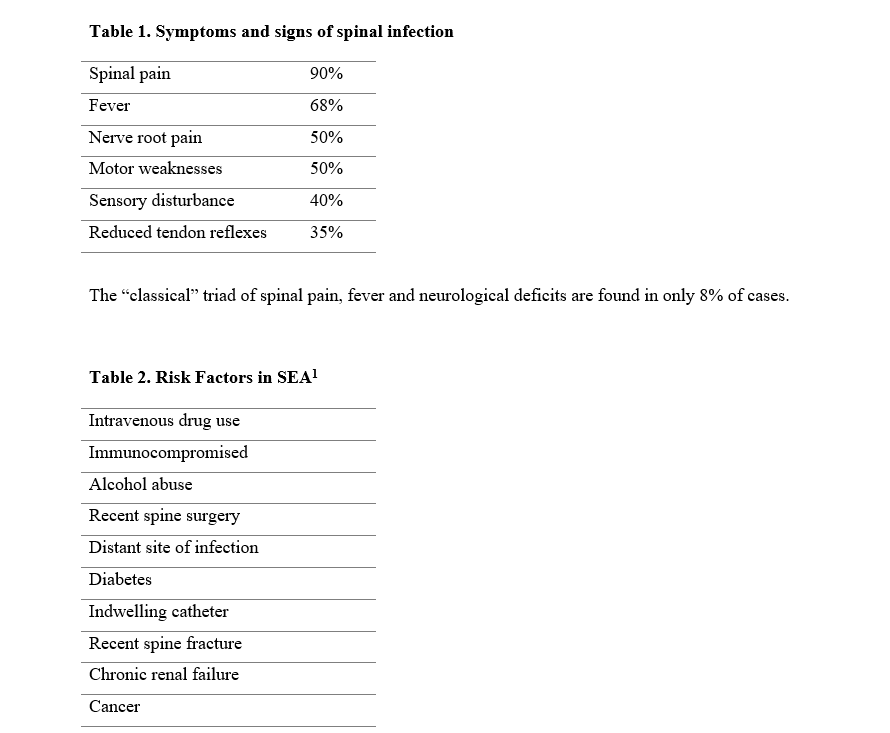
The presence of one or more of the above risk factors are found in 98% of spinal infections.
References
1. Davis DP, Wold RM, Patel RJ, Tran AJ, Tokhi RN, Chan TC, Vilke GM. The clinical presentation and impact of diagnostic delays on emergency department patients presenting with spinal epidural abscess. The Journal of Emergency Medicine. 2004, 26; 26(3):285-291
2. Arko L, Quach E, Nguyen V, Chang D, Sukul S, Kim BS. Medical and surgical management of spinal epidural abscess: a systematic review. Neurosurg Focus. 2014; 37(2):E4
3. Lener S, Hartmann S, Barbagallo GMV, Certo F, Thome C. Management of spinal infection: a review of the literature. Acta Neurochirugica. 2018; 160:487-496
For medico-legal enquiries or to request his CV, Mr Todd can be reached at experts@inneg.co.uk
Tags:
- Paediatric Spinal Surgery
- Spinal Expert Witness
- Informed Consent
- Neuromonitoring
- Causation
- Spinal Infection
Expert Disciplines:
- Neurosurgery
- Orthopaedic Spinal Surgery
About The Author

Mr N V Todd
Consultant Neurosurgeon & Spinal Surgeon
Mr N V Todd is a retired NHS Consultant Neurosurgeon and Spinal Surgeon with expertise in traumatic brain injury, spinal injury, cauda equina syndrome, tumours, stroke, and CNS infections. He has prepared thousands of medico-legal reports and regularly gives evidence in court. He is instructed in roughly 60% Claimant and 40% Defendant cases and has over 130 neurosurgical publications.
From the Blog
Related Articles

Understand how orthotic interventions shape spinal injury rehabilitation outcomes - essential for identifying overlooked care needs, building stronger claims, and maximising compensation accuracy.

Understand why remote spinal assessments risk flawed medico-legal evidence - and why face-to-face exams are vital for defensible, accurate reports in spinal injury and negligence cases.

Gain insights into consent, causation, and breach in complex paediatric spinal claims. A must-read case study for clinical negligence solicitors navigating high-risk surgical decisions.
Find out why 70+ legal firms partner with INNEG.
Request a callback, or contact us.
INNEG respects your privacy. Any information you share with us will be used only to respond to your query.
Phone
+44 161 870 2461Thank you for your request!
We will get back to you as soon as possible.