Through the Keyhole: The Evolution, Risks & Realities of Laparoscopic Cholecystectomy
By Stephen Pollard MA, MS, MB, BS, BSc, FRCS, Consultant Surgeon
Posted 15 December 2025
12 Minute Read

Bile duct injury occurs in up to 0.7% of laparoscopic cholecystectomies - and is one of the most common causes of surgical negligence claims.
Removal of the gall bladder (cholecystectomy) is one of the most performed general surgical procedures with around 66,000 being undertaken each year in the U.K. The first open (i.e. through a full abdominal incision) cholecystectomy was performed in Berlin in 1882, by the German surgeon Carl Johann. Just over a century later in 1985 Prof Mühe of Böblingen, also in Germany, performed the first laparoscopic cholecystectomy using ‘keyhole techniques’ and thus avoiding a major abdominal incision.
When I was working as a Surgical Registrar in Cambridge in late 1980’s I remember the huge excitement when one of the Consultants declared that he was going to attempt to remove a patient’s diseased gall bladder using the keyhole technique without making a laparotomy incision. A full day was set aside for the procedure and the operating theatre doors were taped shut to prevent people other than the operating team entering during the procedure, because of the risk to vision if exposed to the laser that was to be used without appropriate eye protection. This also served admirably to add to the drama and mystique of that first procedure which was surprisingly uneventful, 35 years on, laparoscopic cholecystectomy is now the standard of care for the surgical treatment of gallstones (without lasers) with less visible scarring and quicker recovery and also paved the way for the introduction of laparoscopic techniques for a variety of other general surgical procedures with varying degrees of success (and scepticism).
Most patients with gallstones do not have (or need) surgery in their lifetime, however. Gallstones are very common and are present in 10-15% of adults, rising to around 40% by the age of 60 but we know from post-mortem data that the majority of these were not known about in life and the majority of patients with gallstones actually have no symptoms and require no treatment.
A small proportion of patients with gallstones, however, do develop gallstone related complications and require surgery. An understanding of the anatomy and physiology of the gallbladder is important to appreciate why these symptoms occur, how the surgery is undertaken, and why this commonly performed procedure can lead to litigation. What is unusual about litigation in cholecystectomy is that the most serious cases almost always reflect a failure by the operating surgeon to correctly interpret the biliary anatomy.
Anatomy and Physiology
The gallbladder is a small, pouch-like organ with a muscular wall, which is attached to the undersurface of the liver in the upper right quadrant of the abdomen. Its main function is to store and concentrate bile between meals. Bile is a liquid which is continuously produced and excreted by the liver. Bile contains cholesterol, bile salts and the waste products from red blood cell breakdown, including bilirubin, which is produced from the breakdown of the oxygen carrying molecule haemoglobin which is found in all red blood cells. Bile is also required for the absorption of fats from the intestine.
The bile passes through a series of ducts, leaving the liver through the bile duct which joins the liver to the intestine. A duct coming off the side of the bile duct called the cystic duct leads to the gall bladder. The gall bladder is roughly oval in shape; at the end nearest the cystic duct, it tapers slightly but then widens again before tapering again to join the cystic duct. The slightly dilated segment of gall bladder between the two tapered areas is known as Hartmann’s pouch.
At the lower end of the bile duct, where it enters the bowel, is a nipple like projection called the papilla which is surrounded by a ring of muscle called the sphincter of Oddi (see figure 1) named by Ruggero Oddi, from Perugia, Italy, who described the sphincter in 1887 while he was a medical student.
The common bile duct runs through the head of the pancreas to enter the duodenum. Just before reaching the duodenum the bile duct is slightly wider forming the ampulla of Vater, named after Abraham Vater, a German anatomist who first published a description of it in 1720. The bile duct is joined at the ampulla by the pancreatic duct of Wirsung which drains the digestive enzymes manufactured by the pancreas. Georg Wirsüng gave his name to the pancreatic duct, but it was first identified by his young co-worker Moritz Hoffmann whom it seems was so enringed by this plagiarism that he was the main suspect when Wirsung was murdered in Padua in 1643.
The mixture of pancreatic juice and bile are required for the digestion and absorption of food.
The anatomy of the biliary ductal system shows some variability between individuals. The liver is divided into the right and left lobes. The most frequent anatomical arrangement is that the left lobe of the liver drains bile into the left hepatic duct, and the right lobe of the liver drains bile into the right hepatic duct and the left and right hepatic ducts join to form the common hepatic duct (see figure 1).
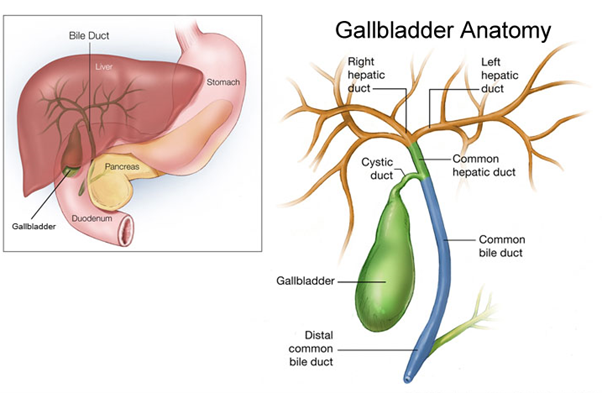
The cystic duct, filling and draining the gall bladder, joins the (patient’s) right hand side of the common hepatic duct which at that point becomes known as the common bile duct. The blood supply to the gall bladder is through a small artery called the cystic artery which usually arises from the right hepatic artery.
Between meals the sphincter of Oddi is contracted, closing off the bottom end of the bile duct and bile preferentially flows along the cystic duct into the gall bladder. The bile is stored in the gallbladder between meals where it becomes more concentrated. After a meal the muscle in the wall of the gallbladder contracts and the sphincter of Oddi relaxes, and as a result the bile contained in the gall bladder is squirted down the cystic duct into the bile duct and, mixing with pancreatic juice in the ampulla, passes through the papilla into the intestine where the bile and pancreatic enzymes mix with food to break it down into components that the body can absorb. It is the bilirubin pigment in bile that gives bowel motions their brown colour.
If the gall bladder is removed, there is no reservoir in the system and bile flows continuously from the liver to the intestine, although the sphincter of Oddi is still functioning and as a result the bile duct often becomes slightly dilated. It also tends to dilate slightly with age but in health it should not be wider than 1 cm. The gall bladder is considered non-essential for health; indeed, some mammals including rats, horses and deer do not have a gall bladder.
Complications of Gallstones
Gallstones are thought to develop because of an imbalance in the chemical make-up of bile inside the gallbladder. In most cases the level of cholesterol in bile becomes too high and the excess cholesterol precipitates gallstones as the bile becomes more concentrated. Less often stones form due to excessive pigment (bilirubin) from increased red blood cell breakdown.
If a gallstone becomes trapped, which usually occurs in Hartmann’s pouch, and blocks the cystic duct through which the gallbladder empties its bile, it can trigger sudden, intense abdominal pain from the obstructed gall bladder. This type of abdominal pain is known as biliary colic or acute cholecystitis. The symptoms will usually settle with antibiotics and time, but unless the stones are removed, it is likely to recur (chronic cholecystitis).
If a small gallstone passes the cystic duct, which is about 5mm across, it can enter the bile duct. Small stones in the bile duct can pass spontaneously through the Sphincter of Oddi but larger ones may not and can then obstruct the flow of bile, causing retention of the yellow bilirubin pigment (which is known as jaundice) and infection of the stagnant bile (cholangitis).
If a small gallstone gets into the ampulla, it can also block the pancreatic duct. Back pressure in the pancreatic duct leads to the release of pancreatic enzymes into the pancreas causing acute pancreatitis which can be manifested just as mild pain but can be severe and even life threatening with severe cases carrying a 15-20% mortality. There are a number of causes of acute pancreatitis, but gallstones and alcohol account for most cases.
Legal point. If a patient suffers acute pancreatitis from gallstones, they need a cholecystectomy performing and for this indication it needs to be performed swiftly, either during the same admission or within 2 weeks of their discharge. I have been instructed in a case which has now settled in favour of the Claimants estate where there was a delay in readmitting a patient for cholecystectomy after being admitted with acute pancreatitis and the patient died from a second episode of pancreatitis having been awaiting cholecystectomy for just over 4 months.
Gall bladder cancer is rare and usually associated with gallstones and the prognosis is poor but there would be a majority body of opinion to support not removing a gallbladder containing stones if asymptomatic, rather than removing it to remove the cancer risk. Like bowel cancer, it is likely that many gall bladder cancers start as benign polyps; the risk of cancer developing in these polyps is directly proportionate to their size. It is not uncommon to pick up polyps when performing ultrasound scans of the gall bladder.
Legal point. If a patient is at an increased risk of developing gall bladder cancer, in particular if they are of Asian or Latin American descent, have a family history of gall bladder cancer and were found to have gall bladder polyp over 1cm in size that was not followed up with serial ultrasound scans, then a case could be made for breach of duty of care if they went on to develop gall bladder cancer.
Investigation of gallstones
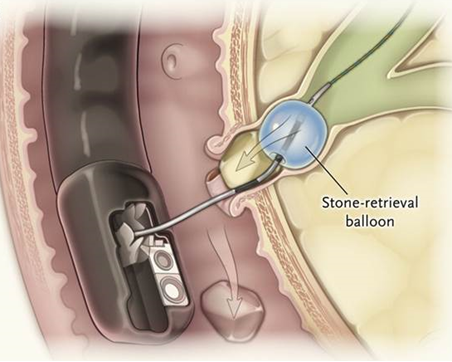
In a patient presenting with indigestion and right sided upper abdominal pain, typically after fatty meals (fat causes the gall bladder to contract), an ultrasound scan is the first line of investigation and will detect most cases of gallstones. It is important to determine at this stage if there are stones in the bile duct as they would not be dealt with during a routine cholecystectomy. Bile duct stones should be suspected if there is a history of jaundice or pancreatitis or a characteristic pattern of abnormal blood tests with a rise in the levels of bilirubin and liver enzyme ‘alkaline phosphatase’ (ALP). 10-18% of patients with stones in their gall bladder have stones in their common bile duct. Bile duct stones may be suspected on an ultrasound scan, either from seeing a stone itself or identifying that the bile duct is abnormally dilated, but the lower end of the bile duct can be difficult to see on such a scan due to overlying bowel gas and if there is suspicion of bile duct stones a more sensitive test is an MRCP (a type of MRI scan), or an ERCP, where an endoscope is swallowed and advanced to the duodenum, and a fine tube passed through the papilla to allow an x-ray to be taken of the inside of the bile duct to show any stones. An advantage of ERCP is that it is possible to extract stones from the bile duct at the same sitting using an expandable wire basket or a small balloon catheter to trawl the duct and extract the stone (see figure 2). The disadvantages of ERCP is that it is more invasive and it does carry a risk of causing acute pancreatitis (which is a recognised complication, not arising from negligence but the patient must be warned about) so should be reserved for cases where is a high index of suspicion of bile duct stones but on occasions patients with claustrophobia cannot tolerate an MRI and ERCP is employed; CT scanning is an alternative but its resolution for bile duct stones is not as good. I have seen a patient death from pancreatitis following an ERCP examination which turned out to be a normal examination and performed because the patient would not have an MRI due to claustrophobia.
Legal point. Ultrasound will correctly identify about 73% of patients suffering from gallstones with bile duct stones, leaving 27% with bile duct stones which have been missed. Normal liver function tests are observed in about 8% of patients with bile duct stones. Providing both tests are done and suggested no bile duct stones, it would not be viewed as a breach of duty of care if they were found subsequently to have bile duct stones (which will be the cases in about 1 in 40 patients) provided there were no symptoms such as a history of previous jaundice/historically abnormal liver function tests, cholangitis or pancreatitis, in which case the index of suspicion should be higher and justify proceeding to MRCP despite currently normal LFTS and a normal bile duct on ultrasound.
Figure 2 Bile duct stone extraction by ERCP
It is normal practice to use an electrified wire to slice across the sphincter of Oddi (sphincterotomy) which is the narrowest point in the system when doing an ERCP for bile duct stones both to allow the basket or balloon to be inserted and also to allow other stones to pass through the papilla (see figure 3).
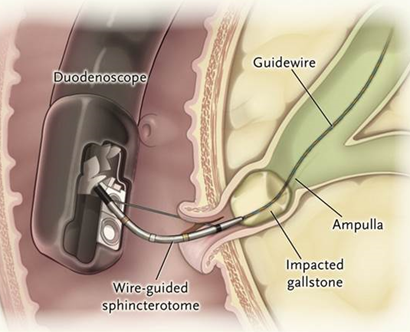
If it is not possible to dislodge a stone which is stuck at the lower end of the bile duct, it is normal practice to insert a fine plastic tube called a stent past the stone to allow the bile to flow past the obstruction.
Legal point. Plastic stents are generally not intended for long term use and generally need to be changed or removed after 12 weeks. If left in the long term they can become encrusted with stones and blocks and lead to obstruction to the flow of bile, pain, jaundice and cholangitis. Imperfect follow-up systems and procedural delays can lead to this occurring but showing breach of duty of care with causation is not clear cut as there is a literature to support long term plastic stenting without stent change or follow-up, particularly in frail or elderly patients who are unsuitable for surgery, unless there was a clearly documented plan for stent removal/ stent change which was not followed. Expert advice in this field should be provided by a medical gastroenterologist with experience of ERCP rather than by a surgeon.
Cholecystectomy
Techniques to dissolve gallstones with bile salt tablets are rarely successful as they require the bile salts (which carry a lot of side effects) to be concentrated by the gall bladder and once diseased by gallstones, the gallbladder rarely functions normally. Breaking stones in the gall bladder with shock wave lithotripsy (unlike kidney stones) have no role as the fragments can pass into the bile duct and cause problems with obstruction or pancreatitis. Treatment of gallbladder stones is surgical and requires removal of the gallbladder with its contained stones. If just the stones were removed, they would reform, so the gall bladder needs to be removed completely. In 90-95% of cases, the surgery is performed entirely laparoscopically (i.e. using keyhole techniques).
Laparoscopic (keyhole) surgery is surgery which is performed using a minimally invasive approach where narrow instruments are introduced into the abdominal cavity through ports inserted through the abdominal wall; surgery is undertaken with the aid of a fibreoptic camera and light source which are also introduced via a port after inflating the peritoneal (abdominal cavity) with carbon dioxide.
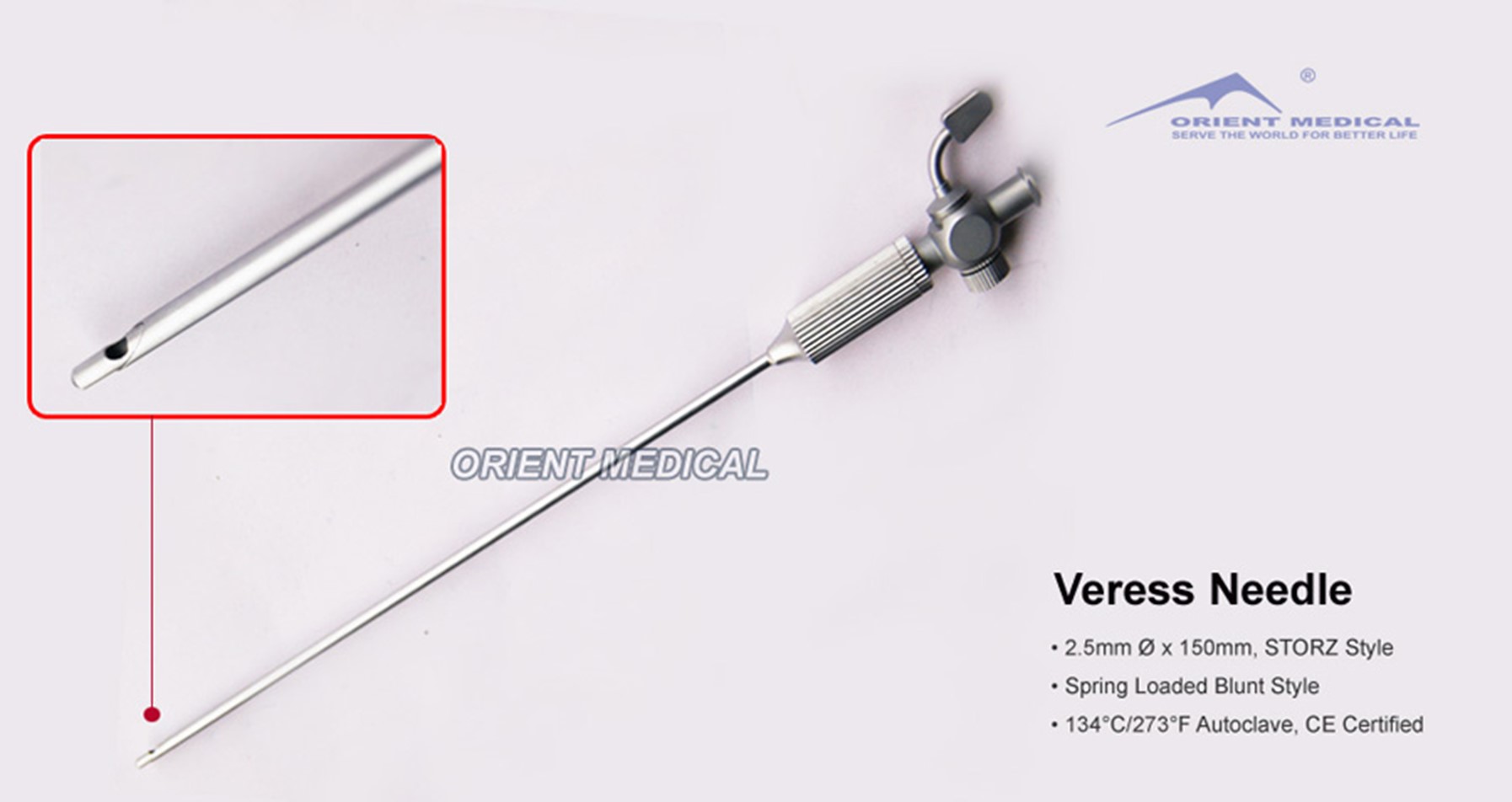
The first stage in a laparoscopic operation is to inflate the abdominal cavity with carbon dioxide to make a space to work in; this can be done in one of two ways. The first is to initially insert a blunt needle (called a Veress needle; see figure 4) into the abdominal cavity well away from any visible scars (i.e. where adherent bowel is least likely to be encountered) and inflate the abdominal cavity with gas (carbon dioxide) via this needle. The Veress needle has a spring-loaded sheath which covers the point as soon as the abdominal cavity is entered.
Figure 4 - Veress needle
The bowel usually falls away, and the gas creates a space between the bowel loops and the anterior abdominal wall into which the laparoscopic ports (to carry the instruments) can then be safely inserted. The second technique is to make a small incision in the region of the umbilicus and insert a port through this incision under direct vision (Hassan’s technique) without using a Veress needle to inflate the abdomen first.
Either way, the first instrument which is inserted is a fibre-optic camera. Once the camera is inserted, everything thereafter is performed under direct vision, observed through this camera (with or without a recording) on a monitor which can be seen by all those present. The camera is inserted through a hollow tube called a port, which is 11-12 mm in diameter (see figure 5).

This hollow port is inserted through a short incision, usually in the region of the umbilicus and is introduced into the abdominal cavity with a sharp metal trocar in the port which is then removed and replaced with the camera which has an integral fibreoptic light source. A variant of this is to use a port with a transparent trocar and with the camera already in the port (known as a Visiport, figure 6) while it is being inserted. Using this technique the insertion route is viewed under direct vision as the point is advanced to reduce the risk of impaling the bowel.
Figure 6 Visiport

Whichever technique is used for the initial instrumentation of the abdominal cavity, the first entry is always to some extent performed blindly. The use or otherwise of a Veress needle for the initial insufflation (which is completely blind) is a personal choice but there is no evidence that this technique increases the risk of bowel injury, and some literature suggests the risk of bowel injury is lower; either technique is acceptable.
Once the camera is safely inside the abdomen further ports can be inserted, whilst looking directly at the entry point from the inside of the abdomen to ensure the trocar does not inadvertently cause any damage. When performing a laparoscopic cholecystectomy, it is usual practice to insert a 10 mm port in the upper abdomen in the midline and two 5mm ports in the upper right side of the abdomen in addition to the camera port.
Legal point. Trocar related bowel perforations during the initial port insertion are a recognised complication of laparoscopic surgery and occur in 0.05-0.5% of laparoscopic procedures and 30-50% are missed at the time that they occur. Perforating the bowel would not be viewed as a breach of duty of care if it was recognised and repaired at the time. If there are adhesions in the region of the initial port insertion, upon completion of the procedure it is important to move the camera to one of the other ports and observe the removal of the first port under direct vision as a perforation may be only become apparent once the port has been removed as the port can act to occlude the perforation preventing the tell-take leakage of bowel contents during the procedure which should never normally be observed. I have taken instruction in several such cases and seen substantial damages awarded for failing to perform this look-back manoeuvre, allowing a bowel perforation to be overlooked.
Trocar injuries to major blood vessels (not including vessels in the abdominal wall) can be lethal and result from the trocar being advanced at the wrong angle and would not normally be defended.
In the early days of laparoscopic cholecystectomy it was common practice to record the procedure on a disc and for this to be retained in the patient’s notes but this is now very uncommon and this just leaves the written operation note as the record of what the surgeon thinks he did ( as is the case with all open procedures). The unique issue about laparoscopic cholecystectomy is that the most serious errors are the result of the surgeon misinterpreting what he has seen and done. When initially evaluating a case it is always worth asking the defendant if there is a video recording available and also asking the defendant or the patient (or their family in the event of a fatality) if there has been an internal enquiry or SUI (serious untoward incident) investigation (often referred to as a Datix) undertaken and the outcome of that investigation as this is often not contained within the patients records. In several cases in which I have been involved the findings of an internal independent SUI enquiry has been sufficient to establish breach of duty of care with admission of liability without recourse to an expert causation report and allow progression to assessment of condition and prognosis.
Although under the duty of Candour the patient or their family should have been informed that such an investigation was to be undertaken, this does not always seem to happen, or if it does the family may not fully understand the process.
Once the camera (laparoscope) is inserted close to the umbilicus and the other ports placed, long handled instruments are used to dissect the tissues of Calot’s triangle, the triangular area bounded by the cystic duct, the bile duct, and the undersurface of the right lobe of the liver /cystic artery (the arterial blood supply to the gall bladder). The cystic artery is divided after being occluded with a metal clip. Similarly, the cystic duct is clipped and divided but only after it has been established that the structure in question is the cystic duct, confirming that it is heading towards the bile duct and that it has no other ducts joining it. The gall bladder is then freed from the liver using electrocautery (diathermy) and extracted through one of the laparoscopic ports having placed it (and its contained stones) in a nylon bag called a Bert bag; if it is not put in this bag it will often split open and shed its stones while being pulled through the narrow incision.
Legal point. If the gallstones are shed into the abdomen during a cholecystectomy, although it is normal practice to try to recover them, it would not be viewed as a breach of duty of care if some were left behind as surgical teaching is that it is acceptable to leave gallstones free in the abdominal cavity.
The greatest hazard when performing a laparoscopic cholecystectomy is to damage the bile duct, usually because of dissecting in the wrong area, inappropriate use of diathermy too close to the bile duct (resulting in a thermal injury) or mistaking the bile duct for the cystic duct. It is observed to occur in 0.3-0.7% of cases of laparoscopic cholecystectomy. It has been demonstrated that the primary cause of bile duct injury is the misinterpretation of biliary anatomy which occurs in 71%–97% of cases.
Over the years, various methods have been proposed and described in the medical literature to prevent iatrogenic bile duct injury. The “critical view of safety (CVS)” technique was introduced by Strasberg in 1995, and it is considered the gold standard to perform a safe cholecystectomy with identification of biliary structures during dissection. CVS was conceived not to perform a laparoscopic cholecystectomy but to avoid biliary injury.
Three criteria are required to achieve the CVS:
- the hepatocystic triangle (Calot’s triangle) must be cleared of adipose and fibrotic tissues; the CBD and CHD must not be exposed;
- the lower third of the gallbladder must be separated from the liver bed to expose the cystic plate (the flat fibrous surface of the liver to which the gallbladder is attached); and
- two and only two structures should be seen entering the gallbladder.
Once these 3 criteria have been fulfilled, CVS has been attained (see figure 7,).
Figure 7 – the critical view of safety as viewed through the laparoscope
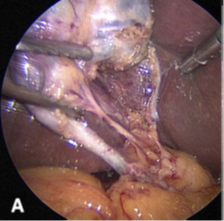
The triangle of Calot has been dissected free of fat and fibrous tissue, however, the common bile duct has not been displayed. The base of the gallbladder has been dissected off the cystic plate, and the cystic plate can be clearly seen. Two and only 2 structures enter the gallbladder - cystic duct to the left (one arrow), and the smaller cystic artery to the right (2 arrows)
Using the CVS technique, the Calot's triangle is completely unfolded by mobilizing the gallbladder neck from the gallbladder bed of the liver. When this view is achieved, the two structures entering the gallbladder (cystic duct and cystic artery) can be definitively identified and divided. It is not necessary to see the CBD since such a procedure may damage the blood supply to the bile duct.
If the surgeon is struggling to correctly interpret the anatomy and identify the cystic duct, there are several strategies which can be employed to prevent bile duct injury. If the surgeon thinks he has identified the cystic duct but is not sure, he can confirm this using an intra-operative cholangiogram (IOC). This is an x-ray performed during a cholecystectomy in which contrast is injected through a fine tube in the cystic duct to confirm that the biliary anatomy has been correctly interpreted. IOC is also used to look for stones in the bile duct if there was any persisting doubt about bile duct stones.
If the bile duct is inadvertently damaged, you cannot simply sew the two ends back together without any chance of success. Firstly, this would not be possible without creating tension on the new joint, and secondly often these injuries are caused by inappropriate use of diathermy electrocautery, and this often causes more extensive tissue damage than is at first apparent. The technique of bile duct repair involves joining the upper end of the bile duct, upstream from any damage, to a loop of intestine which has been isolated from the flow of food by dividing the bowel and reconnecting the upper end of the bowel to the side of the lower bowel to make a Y configuration. This reconstruction has other applications in surgery and is named after the Swiss surgeon Cesar Roux who first described the technique (figure 8).
Figure 8 – Roux-en-Y reconstruction
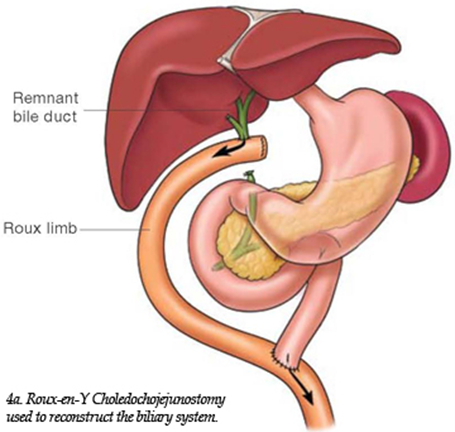
Most of such repairs are successful, but 10-20% go on to develop a stricture (narrowing) of the join between the bile duct and the bowel which causes obstruction to bile flow, jaundice and cholangitis. Although this might be amenable to being dilated radiologically a proportion are refractory to this and require further surgical intervention, which is always very challenging and some will go onto to develop back pressure damage to the liver culminating in secondary biliary cirrhosis for which the only treatment is a liver transplant.
Legal point. Bile duct injury during cholecystectomy is a serious injury which is always avoidable and rarely defensible as it reflects an error in the way in which the surgery was conducted and the anatomy interpreted. The incidence of bile duct injury more than trebled with the advent of laparoscopic cholecystectomy and a common fault made by surgeons is to persist with attempting to complete the operation laparoscopically rather converting to an open procedure or even abandoning the operation while it is still safe to do so. It is surprising how often a surgeon may persist with a difficult laparoscopic cholecystectomy without seeking senior help and/or converting to an open procedure (the same is true of laparoscopic appendicectomy). There is a complicated classification of bile duct injuries (Strasberg-Bismuth classification) based on their location and severity, but this only affects condition and prognosis and quantum of any claim.
Laparoscopic cholecystectomy is within the repertoire of most general surgeons. Repairing a bile duct injury caused during this operation however is specialist hepatobiliary surgery and this expertise may not be available in their own hospital. It would not be regarded as a breach of duty of care to undertake a cholecystectomy without having the skill set to undertake a bile duct repair, but it is essential that a patient is referred to a specialist hepatobiliary surgeon as soon as a bile duct injury is recognised. If this is at the time of surgery, there are occasions where the specialist will travel to the hospital and undertake an immediate repair or give ‘damage limitation’ advice and arrange urgent transfer to their own unit. If a surgeon without appropriate training makes an unsuccessful attempt to repair the injury they have caused, making subsequent management of the bile duct injury more difficult, this would act to further add to the value of the claim.
In a case of a bile duct injury during laparoscopic cholecystectomy in which I am instructed as the Claimant’s expert, following my causation report a very quick without prejudice part 36 offer (‘in full and final settlement’) was made by the defendant. Although my instructing solicitors were tempted to accept it, I was asked my advice and obtained the Claimant’s up to date medical records and discovered that since my causation report she had recently had two admissions with jaundice and cholangitis due to a stricture and it was agreed that they would reject this offer as the quantum of the claim would be much greater now that it had become apparent that there were ongoing problems as a direct result of the injury.
The impact of politics and Covid19
Traditional teaching had been that if a patient was admitted to hospital with acute cholecystitis, they would be managed with pain relief and antibiotics until the pain settled and allowed home to be readmitted some 6 weeks later for cholecystectomy once the inflammation had settled down and the gall bladder was easier to remove. With time however this viewpoint was challenged as it became apparent that if the patient underwent surgery swiftly after admission it was possible to safely complete the surgery and this became the standard of care in many units with the advantage of avoiding a second admission and the potential for readmission with a further flare up whilst waiting although concerns were raised by management as they lost out on the double tariff of an acute admission followed by an elective operation if it was all wrapped up in one patient episode!
What changed everything in June 2019 was the Covid 19 pandemic. Operating theatres became makeshift Intensive Care wards and with no vaccines or quick turnaround tests available all but emergency surgery where there was risk of loss of life, loss of limb or loss of sight effectively came to a standstill. Laparoscopic procedures which were deemed ‘aerosol generating’ were initially banned and guidelines from the Royal College of Surgeons advised that both appendicitis and cholecystitis were to be treated initially with antibiotics and only if they failed to settle then surgery should go ahead but as an open rather than a laparoscopic procedure.
Legal point. I saw a number of patients in my own practice come to harm as a result of this policy including one lady who nearly died from complications of an ERCP which was only required because we could not treat her gallstones in a timely fashion when she presented, and which went on to cause bile duct occlusion some 6 months after her initial admission. I have had several approaches exploring the possibility of litigation for events during this period, but these would be successfully defended based on national policy in place at the time, even though in ‘normal times’ the management would not be of an acceptable standard. In addition, this policy led to a truly massive backlog of work which is still problematic as the time of writing this piece.
Other Complications
While bile duct injury is by far the most important complication in terms of litigation, it is important to consider other post-operative scenarios which are of relevance in this context.
A proportion of patients (which might be as high as 10%) suffer ‘post cholecystectomy syndrome’ which is persistence of their symptoms after the gall bladder has been removed despite the surgery being performed correctly. There is a condition called biliary dyskinesia with pain which mimics gallstone pain but in the absence of gall stones, either in the gall bladder or the bile duct. This is an indication for cholecystectomy even though the gall bladder and biliary tree appear normal. Biliary dyskinesia is also recognised as a cause of persisting pain after the gall bladder has been removed for stones. Inevitably if patients are no better after their surgery they might be expected to seek legal advice as to whether their treatment was substandard but it is actually uncommon to see litigation related to this condition but it is particularly important to ensure patients have been warned of the risk of continuing symptoms where the gall bladder is being removed, particularly if there are no stones.
Legal point. Although post cholecystectomy syndrome is usually non-negligent, there are scenarios which can lead to persisting symptoms which may be labelled as post cholecystectomy syndrome, but which have a physical basis which would be shown to be a breach of duty of care but only if they get investigated.
In legal terms there are two scenarios of post cholecystectomy syndrome where there would be grounds for breach of duty of care; the first is if reasonable steps had not been taken to confirm that the symptoms were due to gallstones/biliary dyskinesia if the symptoms were atypical and an alternative diagnosis was subsequently demonstrated, such as peptic ulcer disease and gastro-oesophageal reflux. If the symptoms persisted but further investigation (even if it should have been done prior to the cholecystectomy but was not) fails to demonstrate an alternate pathology the pain would still be labelled as post cholecystectomy syndrome with no legal case as a result but if subsequent investigations showed pathology which explained the symptoms, the pain suffering and loss of amenity from the unnecessary cholecystectomy could lead to a claim.
The second is where the surgery had not been performed to a reasonable technical standard leading to continuing symptoms. I can give two examples in which I been instructed and damages awarded. In the first case, there were stones in the bile duct which were not recognised pre- or post-operatively due to the patient not having appropriate tests (in this case the liver function tests were not done although being requested and this was not picked up) which would, on the balance of probabilities, have indicated that bile duct stones could have been present. In a second case the gall bladder was not removed completely, and Hartmann’s pouch and its contained stones had remained. I suspect the junction of Hartmann’s pouch, and the gall bladder was mistaken for the junction of Hartmann;s pouch and the cystic duct. The ongoing pain was labelled as post cholecystectomy syndrome for some months until a stone entered and occluded the bile duct and an ultrasound scan showed the stone filled gall bladder remnant; the patient required a second cholecystectomy and an ERCP and appropriate damages were awarded.
Issues of Consent
Cholecystectomy is an operation that is performed so frequently that many units have printed information leaflets in addition to what is put on the consent form. These leaflets might have been produced in house or might be generic such as those produced by EIDO, who provide information for informed consent for about 400 procedures (https://www.eidohealthcare.com/)
Patients undergoing laparoscopic cholecystectomy must warned of the risk of bile duct injury and bile leak. It is an important point that warning of the risk of bile duct injury is essential but should such an injury occur the fact that this is a recognised complication and that they have signed the consent form does not mean it would not be a breach of duty if it were to occur. Bile leaks when not due to damage to the common hepatic duct or the common bile duct are less serious and infrequently require major surgery and can arise due to leakage from small accessory ducts in the gall bladder bed and from the cut end of the cystic duct if it is not properly secured. Sometimes patients suffer a bile collection in the gall bladder bed, and no cause is found. In the majority of cases of bile leakage where the bile duct is intact, breach of duty of care will not be shown and as most will resolve swiftly with a laparoscopic washout +/- an ERCP the quantum for such claims would be small but if there is a persistent bile leak or if major corrective surgery is required it is worth exploring the cause.
It is also important that patients clearly understand that there is always the possibility of open conversion, as this will require a 3-5 day stay in hospital (laparoscopic cholecystectomy is usually performed as a daycase) and a longer recovery period as well as a longer scar and a greater risk of wound related complications.
Since around 10% of patients will experience ongoing biliary pain after a correctly performed cholecystectomy and a similar number will develop loose stools after cholecystectomy, although they would not be shown to reflect a breach of duty in the conduct of the procedure, it is important that they appear on the consent from although in my own experience I have never known a patent to not go ahead with surgery when warned of these risks.
New Developments
For completeness I should mention two areas of evolution of laparoscopic cholecystectomy.
Although the scarring from a laparoscopic cholecystectomy is very minor, there are ‘pioneers’ who have sought to lessen it further. I personally was totally comfortable with the standard laparoscopic cholecystectomy and chose not to engage with these two new techniques but I thought it would be interesting to mention them.
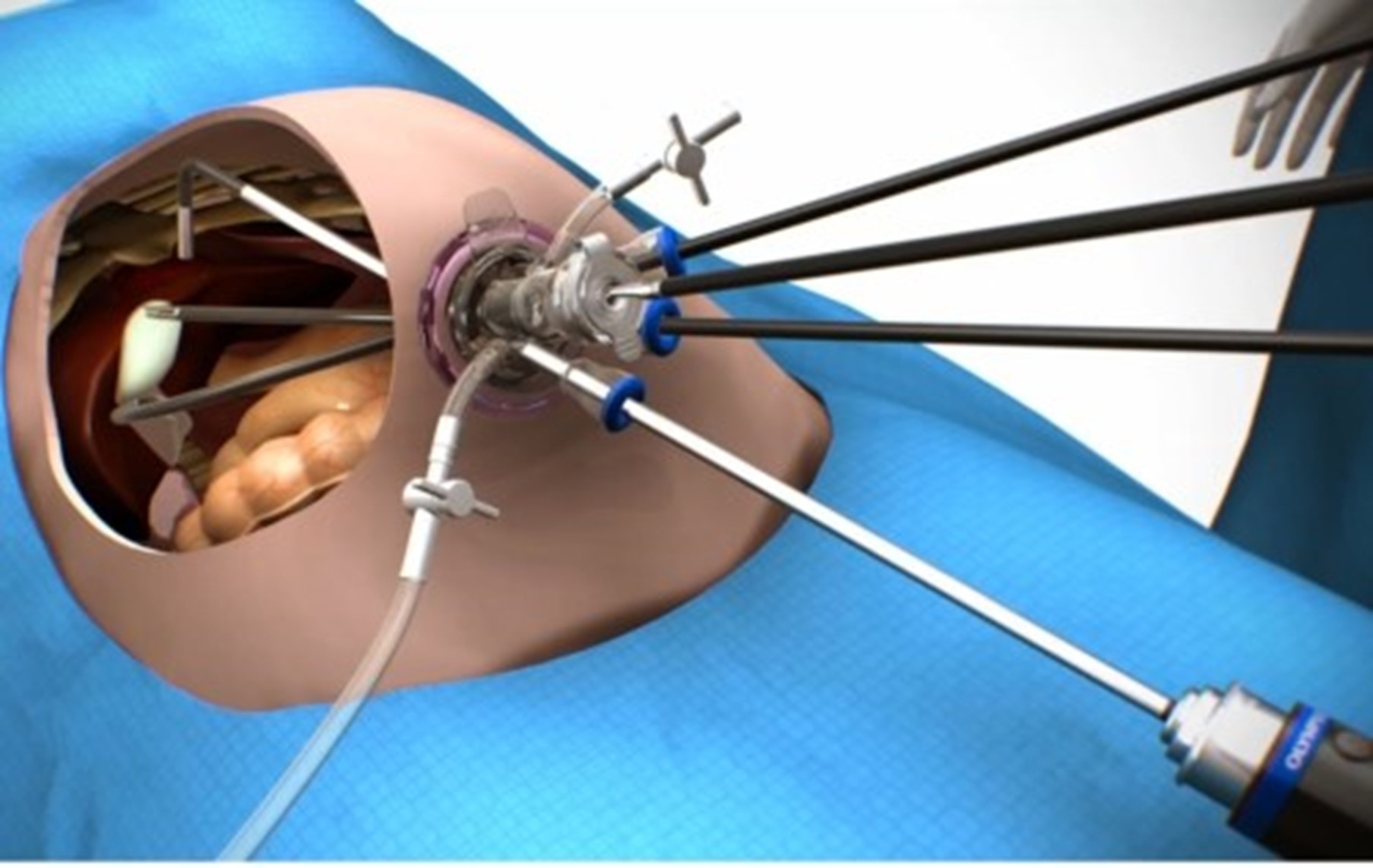
The first was using the SILS technique (single incision laparoscopic surgery) where all the instruments as well as the camera are passed down a single port placed through the umbilicus (see figure 9).
Figure 9 - SILS technique of cholecystectomy
It seems however that even the scar in the umbilicus is too much for some people and in around 2007 I was told about a well-known supermodel who had had her gall bladder removed through her vagina thus leaving no visible scar at all. I was waiting for the punchline until I realised that it was true and there is now a select group of surgeons undertaking natural orifice transluminal endoscopic surgery (NOTES) which is performed either through the roof of the vagina or through the wall of the stomach or through the rectum. (see figure 10).
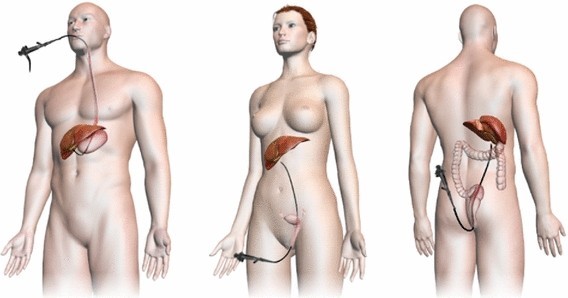
Personally, I would have thought that there was significant and unnecessary potential for complications when making and closing holes in the vagina, stomach or intestine and the uptake of NOTES is relatively small but there is a dedicated group of very skilled surgeons who think this is the way ahead. For me however, it recalls this Farside cartoon!
Explore more medico-legal insights from leading surgical experts - read our latest webinars and case analyses here >
Tags:
- Informed Consent
- Expert Panel
- Delayed Surgery
- Clinical Negligence Experts
- Bladder Injury
Expert Disciplines:
- General Surgery
About The Author

Stephen Pollard MA, MS, MB, BS, BSc, FRCS
Consultant Surgeon
Mr Stephen Pollard MA, MS, MB BS, BSc, FRCS, was appointed Consultant Surgeon in 1993. His specialist interests include adult liver and kidney transplantation and bariatric surgery. After a fact-finding visit to Richmond, Virginia, in 1994, he established one of the UK’s first multi-disciplinary bariatric teams and was a founding member of the British Obesity and Metabolic Surgery Society (BOMSS). Working alongside Peter Lodge, he helped perform some of the world’s first intestinal and multivisceral transplants.
From the Blog
Related Articles

Understand the key drivers behind delayed colorectal cancer diagnoses and how they translate into clinical negligence claims - essential insight for solicitors navigating diagnostic failures and missed referrals.

Functional Neurological Disorder (FND) is one of the most frequently misdiagnosed and misunderstood conditions in medico-legal practice...

Gain crucial insights on complex consent and surgical risks in paediatric spinal cases to strengthen your clinical negligence claims and better support vulnerable patients and their families.
Find out why 70+ legal firms partner with INNEG.
Request a callback, or contact us.
INNEG respects your privacy. Any information you share with us will be used only to respond to your query.
Phone
+44 161 870 2461Thank you for your request!
We will get back to you as soon as possible.